
In the previous article I wrote about how bad the motion palpation tests are for assessing the SIJ. So, what tests are actually good for assessing the SIJ joint then?
The only tests that actually are useful for SIJ testing are joint provocation tests. Research shows that provocation tests both tests intra- and extra articular tissues, and it’s impossible to separate the two with physical examination (1). There are only two studies that are of higher quality according to Han et al (2), and that is the study by Laslett et al. (3) and van der Wurff et al. (4).
Laslett cluster
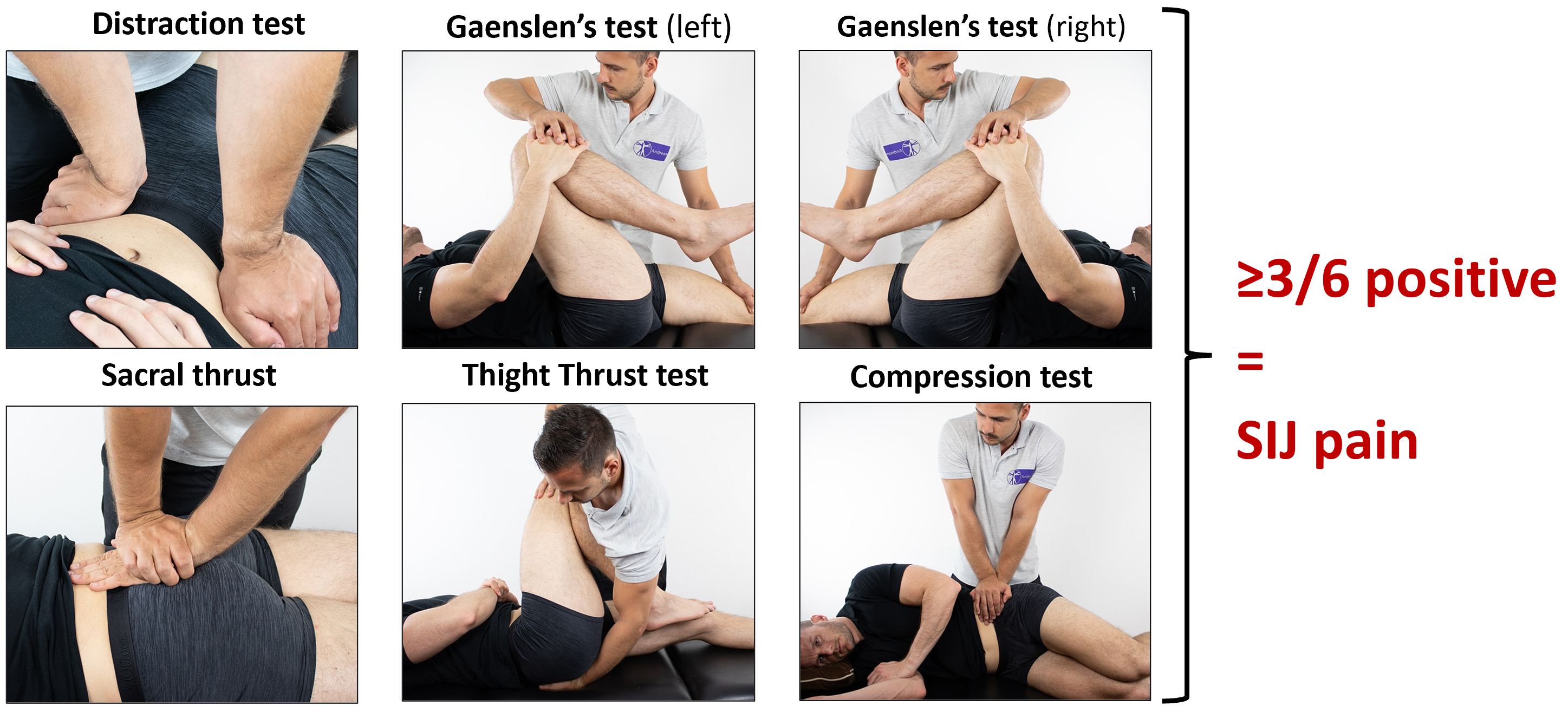
That’s why we usually talk about the “Laslett cluster” when it comes to SIJ testing (3). Laslett, with others, compared SIJ provocation tests with injection of the joint. Out of six tests, three or more positive tests are of value in clinical diagnosis of a symptomatic SIJ (5). Sensitivity and specificity were 91 % and 78 % respectively. Remember SpIN (specificity rules in) and SnOUT (sensitivity rules out), meaning the tests are a bit better at ruling OUT than IN. They state that when all provocation tests are negative you can rule out pain coming from the SIJ (5).
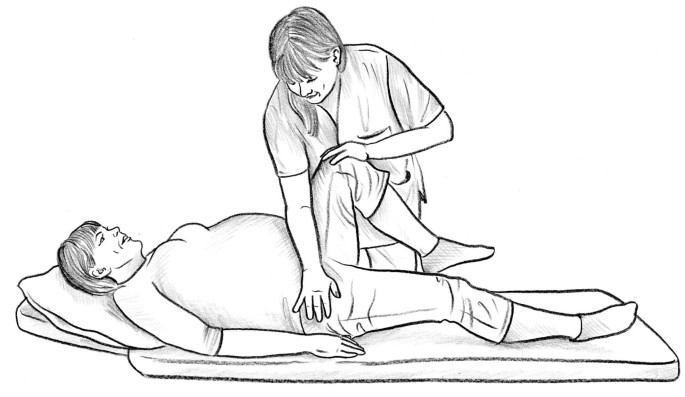
These are the tests (there are 5 tests, 6 in total, because you do both sides with Gaenslen’s – it has the potential to provoke both sides, from my understanding):
You can also see how to do them here:
Centralisation or peripheralisation?
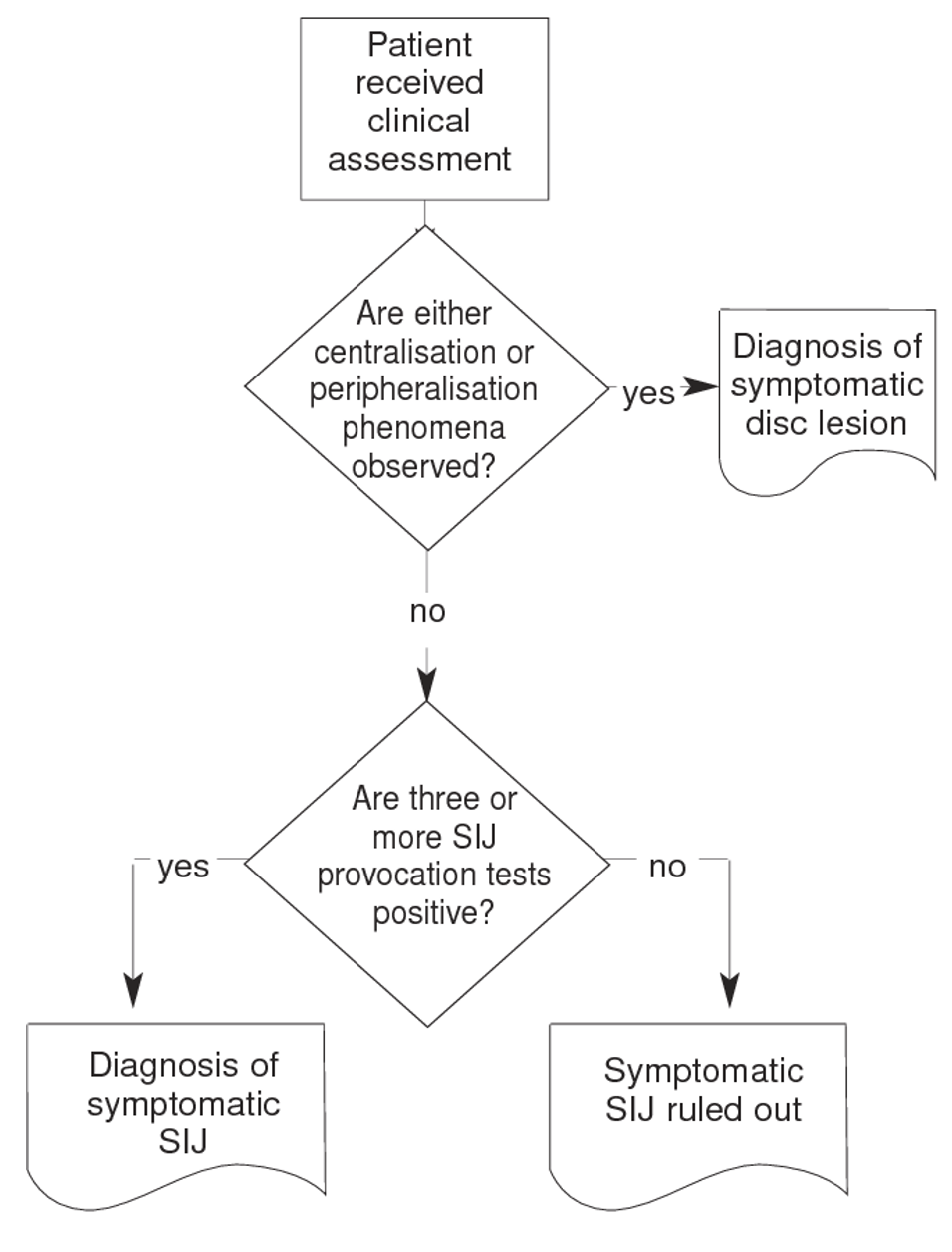
In the original article from 2003, an important aspect of getting these results was to rule out the pain coming from the back by using the McKenzie principle (Mechanical Diagnosis and Therapy (MDT) looking for the centralisation or peripheralization phenomena – meaning that repeated movements for the spine in flexion, extension and/or lateral flexion moves the symptoms closer or further away from the centre of the spine.
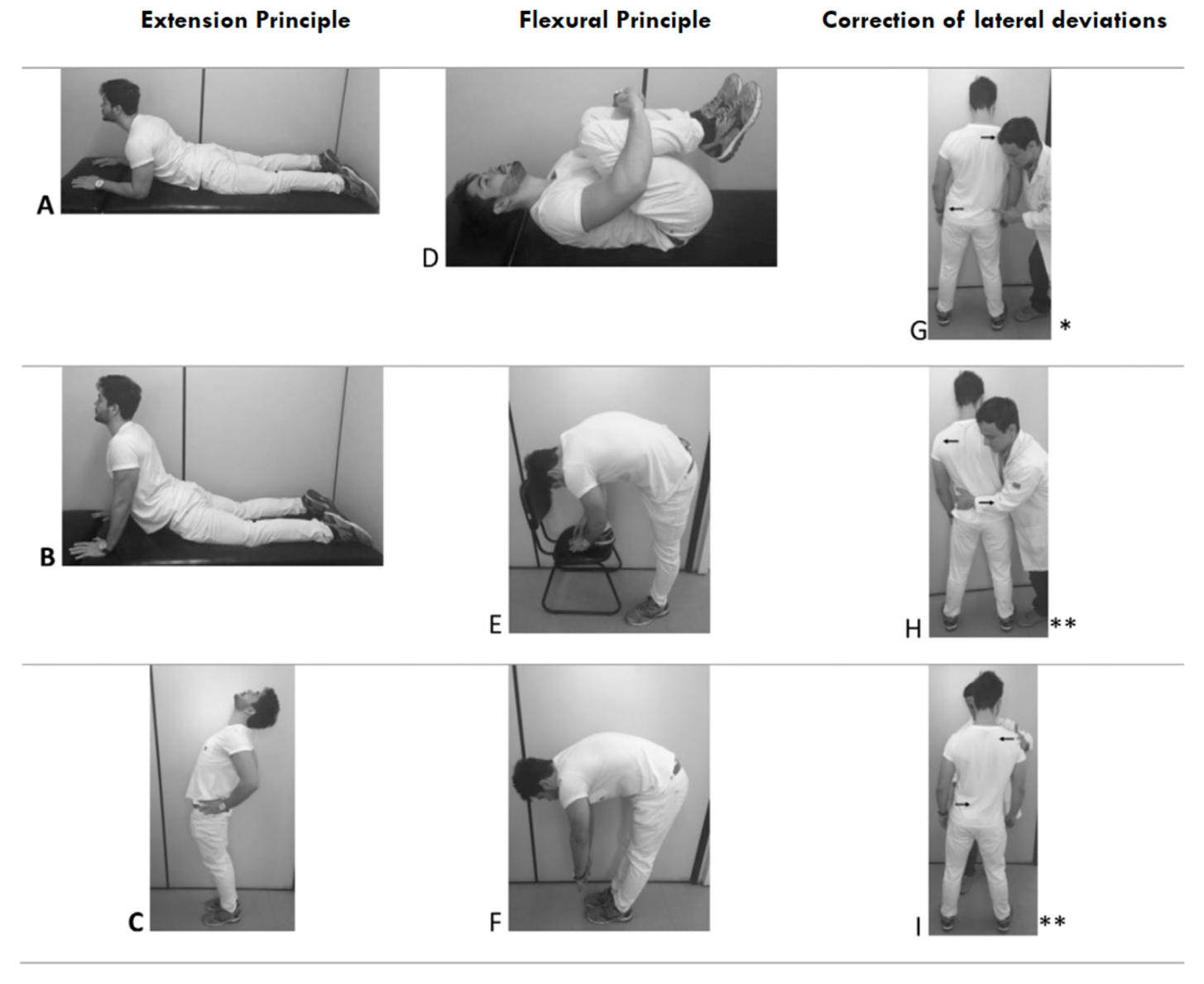
If they saw that the pain changed in either direction they concluded that the pain was coming from the spine – most likely the disc (3). Only including the patients that didn’t have centralisation or peripheralization phenomenon increased the specificity from 78% to 87%, while the sensitivity remained at 91% (7).
I am not a McKenzie therapist myself (I don’t put my trust purely in to one concept, if you can say it’s a concept?), but here are a few examples on how to test for directional preference (centralisation and peripheralisation), if you want to see how it might look: https://youtu.be/ShM14BoX2WE?si=xcbYdI62_1JTuhsk
On a sidenote, there are a lot of opinions about the McKenzie principle, and whether you can diagnose disc related back pain (more about this in another post?). In Norway the courses were very popular 10-15 years back. I haven’t done a course with the McKenzie people myself, but I like the idea with a systematic assessment. And I do agree – if the symptoms change because you move the spine, maybe it’s actually coming from the spine? Still, it is debatable whether you can be specific on the structure, and whether it actually matters for the treatment.

Personally, I think taking bits from here and there and using what fits best for the patient in front of you, I think is key. I, myself, have “stolen” the parts I like from other “concepts” or ideas. In my treatment I might use elements of:
- directional preferences (McKenzie?)
- cognitive functional therapy (breathing, relaxed movements vs tense)
- mobilisation with movement (Mulligan?)
- cervical spine mobilisation (Kaltenborn)
- cognitive therapy (challenging patient’s belief in a non-threatening, ideal manner)
- exercise (traditional strength training, plyometric, aerobic, balance etc)
- ways of communicating (brief intervention, metaphors from courses, mentors, things I’ve read)
- and yes, sometimes even a lumbar spine manipulation (if the patient really wants it, and we’ve ruled out risky stuff) (would that be Maitland?).
I don’t think sticking to one concept is the best way to do things, I think we need to be flexible when it comes to intervention strategy.
Anyways, back to the SIJ testing.
You might just need to do two SIJ tests
Laslett et al did further analysis on the SIJ tests. In their paper from 2005 they took another look at testing algorithms, and they didn’t include the need of looking for directional preference (centralisation or perpiheralisation). They saw that the most sensitive test is the thigh thrust test (88%), and distraction test is the most specific (81%).
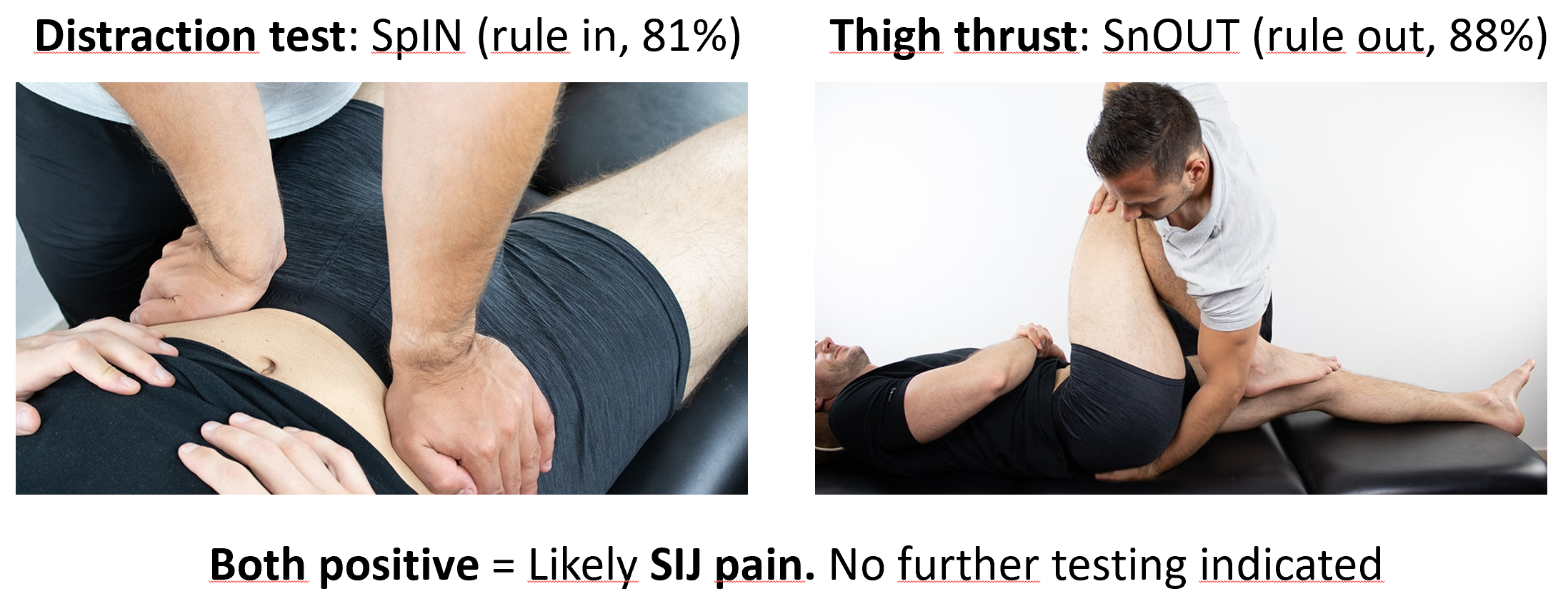
The thigh thrust rules out, the distraction test rules in. Therefore it is recommended starting with these two. If both these tests are positive no further testing is indicated (5). If one is positive you can continue doing further testing. Below is the algorithm that Laslett has suggested (5). This means you can skip the Gaenslen’s tests. Gaenslen’s test is probably the one I dislike the most, as you have to shift the patient over to the sides of the treatment table on both sides, and this can be painful if you have hip pain. If the patient has a lot of pain it can be quite hard for them to do, and it takes time.
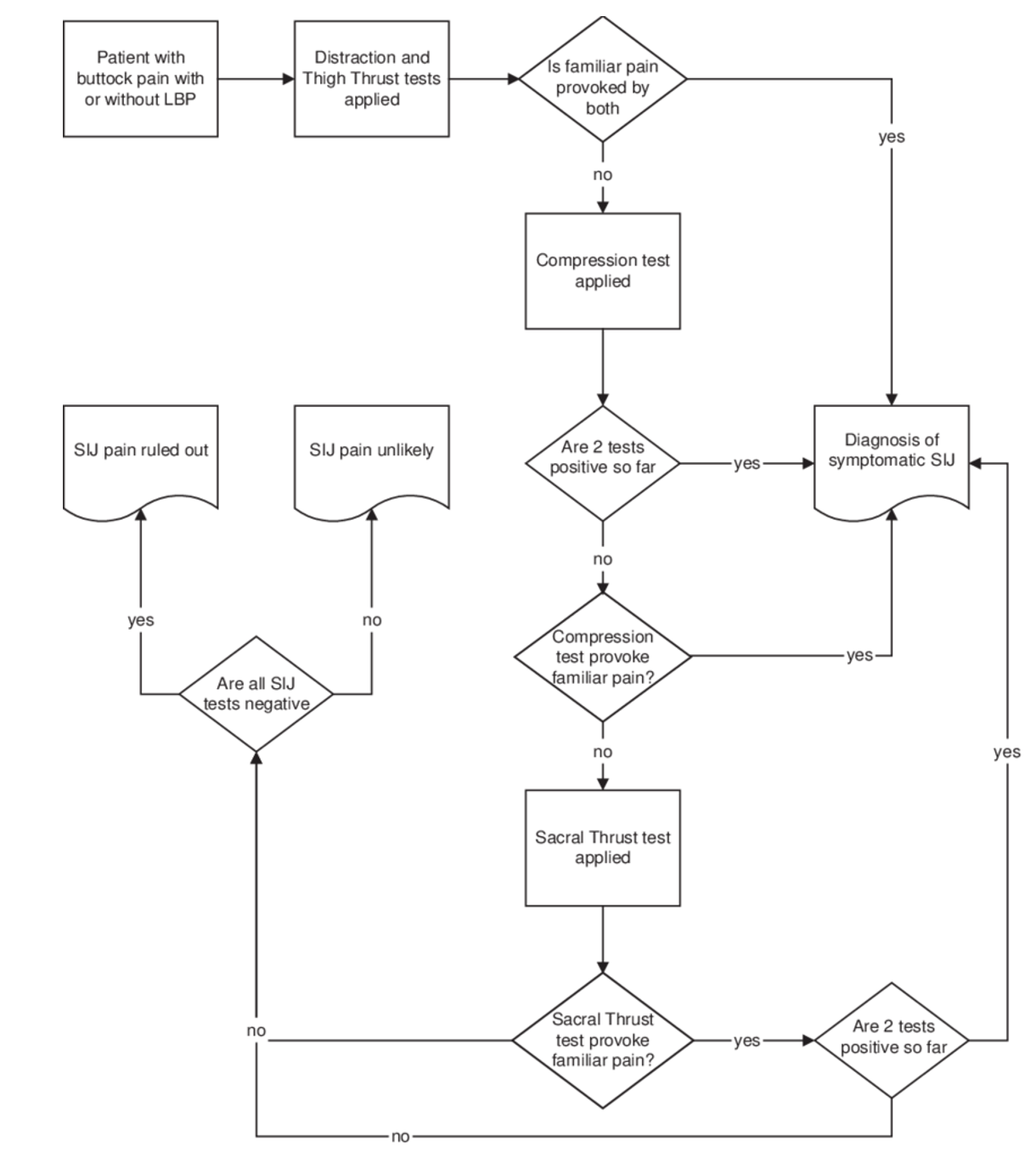
Again, if all SIJ tests are negative you can confidently rule out SIJ pain.
van der Wurff cluster
The second study with high quality is the one by van der Wurff et al (4). They also found that three or more positive tests was indicative of SIJ pain. They did the same as Laslett, except they did FABER instead of sacral thrust test:
- Distraction test
- Compression test
- Thigh thrust test
- Patrick’s (FABER) sign
- Gaenslen’s test
There are lots of ways of doing FABER test. Some people put the foot on top of the other leg. I do it like this, which is also what is instructed in the original paper (4,8).

In the study by van der Wurff they followed the instructions made by Kokmeyer (8), and they only tested Gaenslen’s on the affected side, meaning the side where the leg goes out of the table.
van der Wurff et al. would like to emphasise that ruling out SIJ pain (less than 3 positive) is very useful, since it avoids further unnecessary investigations or treatments.
Beware of false positives
As is stated in Laslett’s article, you should be aware of false positives if the patient has got high levels of pain with all body movements (disc herniation, fractures etc.) (5). Most likely all tests will be painful, and in these cases, interpretation of SIJ tests is inappropriate. Looking at this, in 2020 there was a study showing that 33 % of people with disc herniation tested positive for SIJ pain (3 or more positive tests) (9). Funny enough (!) they did not even discuss the possibility for false positives. Because disc herniation and radicular pain can be very painful! They even saw that the SIJ group scored significantly higher on the LANSS pain scale for neuropathic pain – which tells me even more that these are probably false positives. More neuropathic pain = more painful with all tests.
Just to mess with us a bit, there is a study from Sweden that showed that the posterior pelvic pain provocation test (P4) was negative in patients with lumbar disc herniation and radicular pain. This test is more commonly used to diagnose pelvic girdle pain, and is a tiny bit different than the “thigh thrust test” (you don’t put your hand on their sacrum on the P4, but stabilises the opposite ilium) (10). There might be many reasons for these results in this study. There might have been methodological differences? Or maybe the P4 test provokes less pain for a painful back, compared to a full SIJ test battery?
We will get back to the P4 and the pelvic girdle pain in the next article.
Conclusion
Joint provocation tests are the best to assess for SIJ pain. They are probably better at ruling out, than ruling in. I think it’s important to find a routine that is standardised, that you do well and feel comfortable with, but you must always do a cluster of tests. You can choose from Laslett’s or van der Wurff’s cluster. If you have a high suspicion that this is SIJ pain it can be enough to just do a distraction test and then the thigh thrust test. If these two are positive you know it’s SIJ pain, and you don’t have to do more testing. If you are really pushed on time the thigh thrust test is the best to rule out (88%), even though you shouldn’t rely on one test alone.
References
1. McCormick ZL, Hurley RW, Anitescu M, Bhaskar A, Bhatia A, Cassidy RC, et al. Consensus practice guidelines on sacroiliac joint complex pain from a multispecialty, international working group. Pain Med. 2025 Dec 1;26(12):817–917. doi:10.1093/pm/pnaf129 PubMed PMID: 41318933; PubMed Central PMCID: PMC12681192.
2. Han CS, Hancock MJ, Sharma S, Sharma S, Harris IA, Cohen SP, et al. Low back pain of disc, sacroiliac joint, or facet joint origin: a diagnostic accuracy systematic review. eClinicalMedicine. 2023 May 1;59. doi:10.1016/j.eclinm.2023.101960 PubMed PMID: 37096189.
3. Laslett M, Young SB, Aprill CN, McDonald B. Diagnosing painful sacroiliac joints: A validity study of a McKenzie evaluation and sacroiliac provocation tests. Aust J Physiother. 2003;49(2):89–97. doi:10.1016/s0004-9514(14)60125-2 PubMed PMID: 12775204.
4. van der Wurff P, Buijs EJ, Groen GJ. A multitest regimen of pain provocation tests as an aid to reduce unnecessary minimally invasive sacroiliac joint procedures. Arch Phys Med Rehabil. 2006 Jan;87(1):10–4. doi:10.1016/j.apmr.2005.09.023 PubMed PMID: 16401431.
5. Laslett M, Aprill CN, McDonald B, Young SB. Diagnosis of sacroiliac joint pain: validity of individual provocation tests and composites of tests. Man Ther. 2005 Aug;10(3):207–18. doi:10.1016/j.math.2005.01.003 PubMed PMID: 16038856.
6. Artioli DP, Bertolini GRF. Método McKenzie na Fisioterapia (Diagnóstico e Terapia Mecânica): Aplicação de Raciocínio Clínico Lógico e Revisão Sistemática. Rev Pesq Fisio. 2018 Sep 17;8(3):368–76. doi:10.17267/2238-2704rpf.v8i3.1965
7. Laslett M. Evidence-based diagnosis and treatment of the painful sacroiliac joint. J Man Manip Ther. 2008;16(3):142–52. doi:10.1179/jmt.2008.16.3.142 PubMed PMID: 19119403; PubMed Central PMCID: PMC2582421.
8. Kokmeyer DJ, Van der Wurff P, Aufdemkampe G, Fickenscher TCM. The reliability of multitest regimens with sacroiliac pain provocation tests. J Manipulative Physiol Ther. 2002 Jan;25(1):42–8. doi:10.1067/mmt.2002.120418 PubMed PMID: 11898017.
9. Telli H, Hüner B, Kuru Ö. Determination of the Prevalence From Clinical Diagnosis of Sacroiliac Joint Dysfunction in Patients With Lumbar Disc Hernia and an Evaluation of the Effect of This Combination on Pain and Quality of Life. Spine (Phila Pa 1976). 2020 Apr 15;45(8):549–54. doi:10.1097/BRS.0000000000003309 PubMed PMID: 31842104; PubMed Central PMCID: PMC7208275.
10. Gutke A, Hansson ER, Zetherström G, Ostgaard HC. Posterior pelvic pain provocation test is negative in patients with lumbar herniated discs. Eur Spine J. 2009 Jul;18(7):1008–12. doi:10.1007/s00586-009-1003-z PubMed PMID: 19390876; PubMed Central PMCID: PMC2899577.
11. Szadek K, Cohen SP, De Andrès Ares J, Steegers M, Van Zundert J, Kallewaard JW. 5. Sacroiliac joint pain. Pain Practice. 2024 Apr;24(4):627–46. doi:10.1111/papr.13338
