The sacroiliac joint (SIJ) sits in a strange place in musculoskeletal care.
Some argue it barely moves and rarely causes pain. Others claim they can feel subtle motion, diagnose positional faults, and “realign” it.
How much of a problem is it really?
If you look in the research it is estimated that 10-30 % of people with axial low back pain have their pain because of nociception from the sacroiliac joint (1,2). I must admit I don’t feel I see SIJ pain as often as that. I remember reading a lot of sceptical articles about the SIJ when I was a new graduate (which were great): How it doesn’t move much and that a lot of treatment is based of false premises (which I do still mainly agree with).
Has this made me ignorant to the SIJ as a cause of back pain, and made me forgotten about it?
About the sacroiliac joint
The sacroiliac joint is a joint that barely moves. The little movement it does is mainly to transfer load between the spine and the legs. It acts as a stress reliever! (1). According to one paper the joint moves 8 mm at its maximum, but averages 2-3 mm (3).
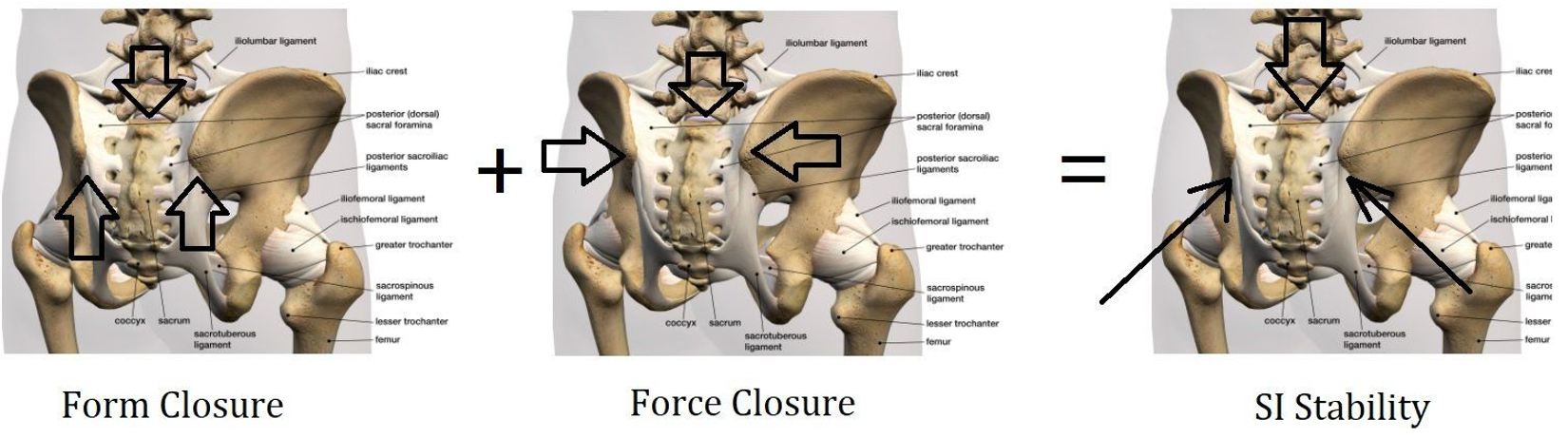
Commonly, a way to explain the joint is by using the terms form closure and force closure.
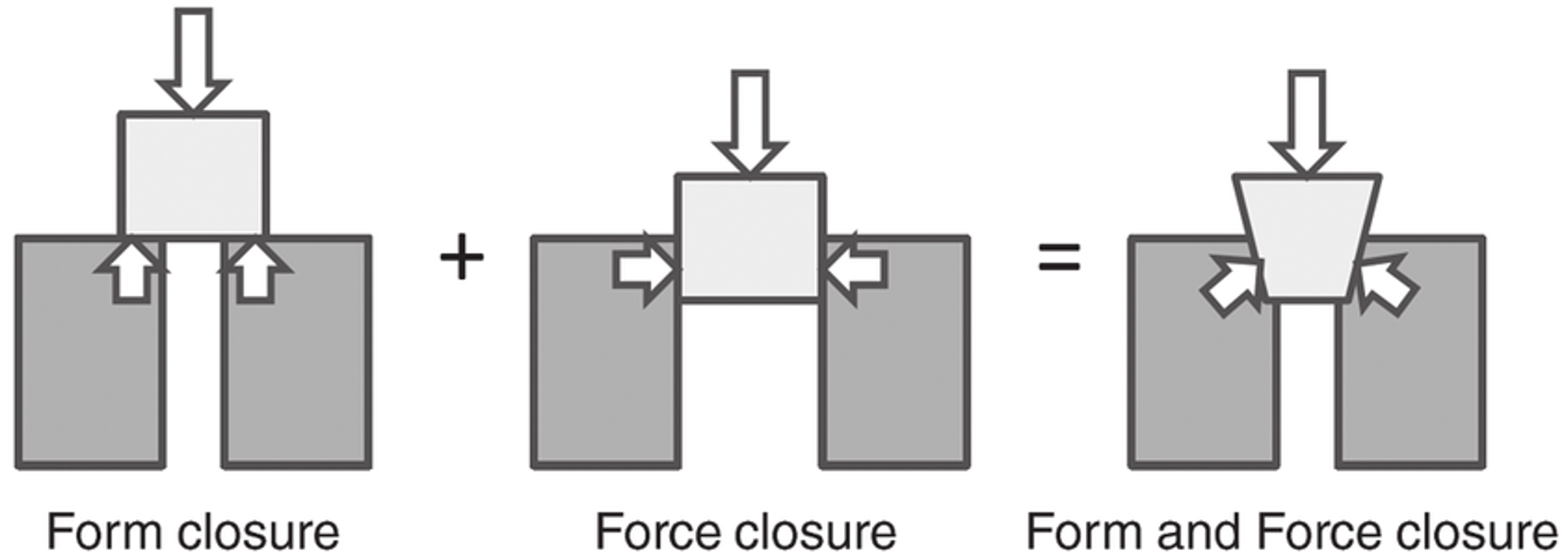
Form closure means how the bones/cartilage fits together. The SIJ fits together well, creating stability (4). Force closure explains how the muscles holds everything together when needed (1). The point here is you need balance between mobility and stiffness (1).
SIJ Complex Pain?
McCormick et al from 2025 argue that we should call it sacroiliac joint complex pain, not just SIJ pain, because there are a lot of other tissues that potentially can be the source of nociception: You have the anterior and posterior ligaments, with capsule and synovial lining. A lot of the research is also done with the help of intra articular injections, but even these can have their limitations, as the S1 foramen is very close and communicate with the joint, and there can be leaks and defects of the capsule. This can give a false positive test outcome (2).
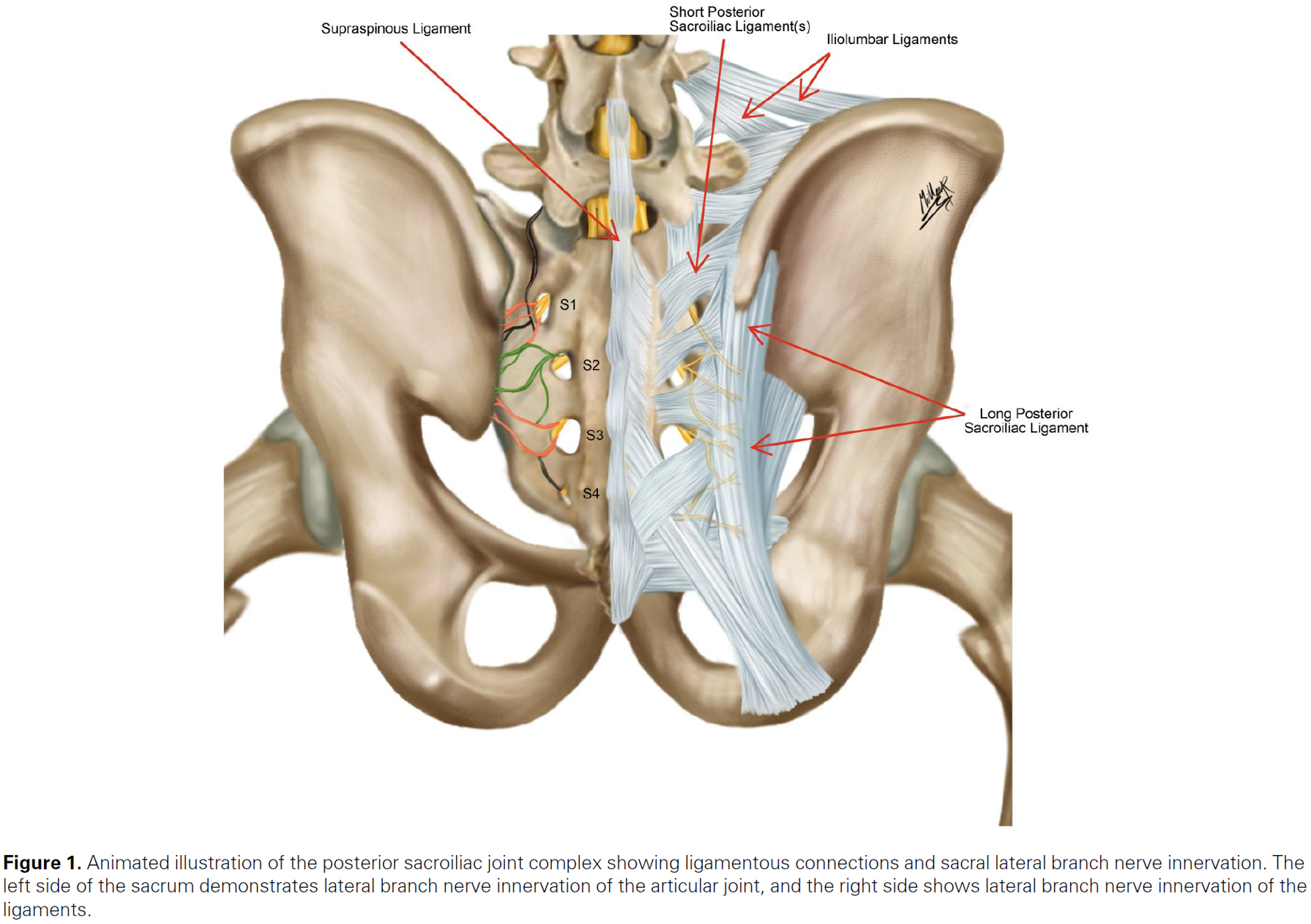
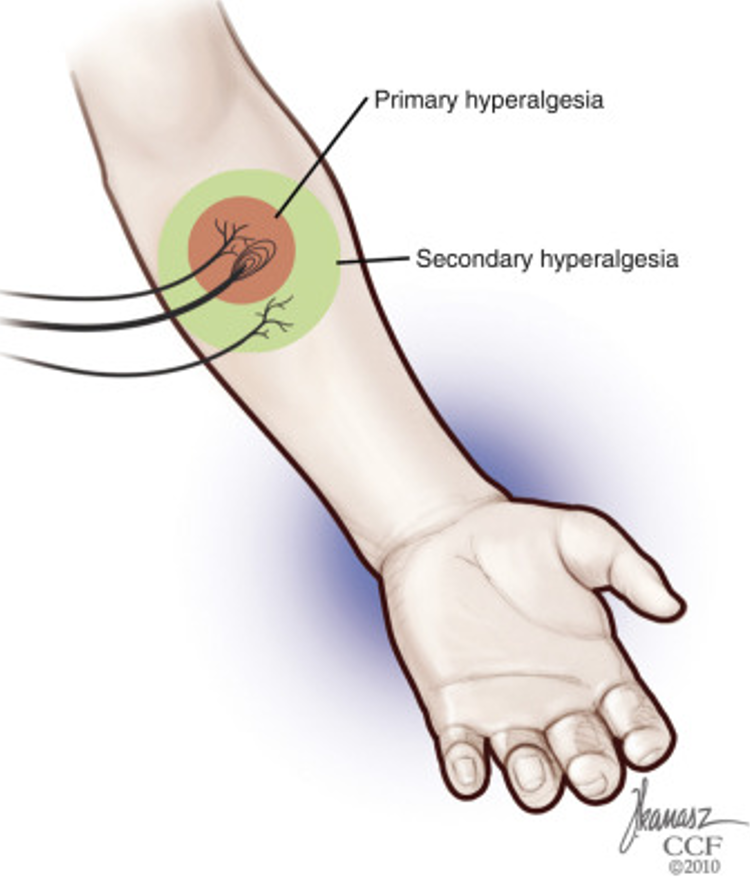
So yes, the nociceptive input can also come from outside the joint. A potential source for extra-articular nociception is the “long dorsal ligament”, also called long posterior sacroiliac ligament. This ligament is anatomically connected to the erector spinae muscle and other structures, and it also shares innervation with the SIJ. According to an article, the long dorsal ligament pain is at least as common as SIJ pain itself (2). It’s more commonly seen with younger people who fall on their buttock (2). I also think it’s important to remember that this ligament can be painful because you have a painful SIJ or low back. Secondary hyperalgesia! If you have pain in the area, it can be painful to palpate the tissues around it!
Who gets SIJ pain?
So who is it that gets SIJ pain? In a retrospective study they looked at patients who responded to an intra articular injection of the SIJ. These patients had a history of vehicle accident, fall on the buttock(s), postpartum state, American football injuries or pelvis fracture. We’re talking high forces injuries (2), not minor movements that might cause the SIJ to “jump out of positions”, as some might have us believe.

Another article mentions SIJ pain being more prevalent in sports as football, basketball, powerlifting, gymnastics, golf, cross country skiing and rowing. Sports that challenge the force closure, typically single leg stance with torsion, e.g. skating, cricket, racket sports can also cause SIJ pain (1). Think running, jumping and landing, probably more with single leg work!
A lot of the times I also think SIJ pain can be a consequence of other things going on, like back pain with bracing and lack of natural movement of the spine. Bracing and a stiff spine might cause irritation in other areas, like the SIJ? “Is it the victim or the culprit”, as Booth said in his article (1)?

You can see the same tendency with patients who has had a lumbar fusion. If some joints move less, maybe other joints need to move more (some would call this “adjacent level disease”). With lumbar fusion the SIJ pain prevalence rates is up to 33-59 % (2), but remember that there might be a lot of things going on with a patient with lumbar fusion (comorbidities, general health, psychosocial factors, complications?).
Another population that can get SIJ pain are women during and/or after pregnancy, presenting with what we call pelvic girdle pain (PGP). This can include both SIJ joints, but also the pubic symphysis (5). More about this in another article.
Not to be missed are the patients having sacroiliitis or SIJ pain because of an underlying rheumatic disease. Axial spondyloarthritis commonly presents with pain around the SIJ. I think it’s important knowing how to screen for this, as average time to get the diagnosis is 8,5 years (6). Also, more about this later.

Where do they have pain?
According to one article the pain would be localised in the buttock and groin on the affected side, but there are some disagreements here (1). Trying to make things a bit more clear you have the famous Fortin who did the research and came up with the “Fortin finger sign”.
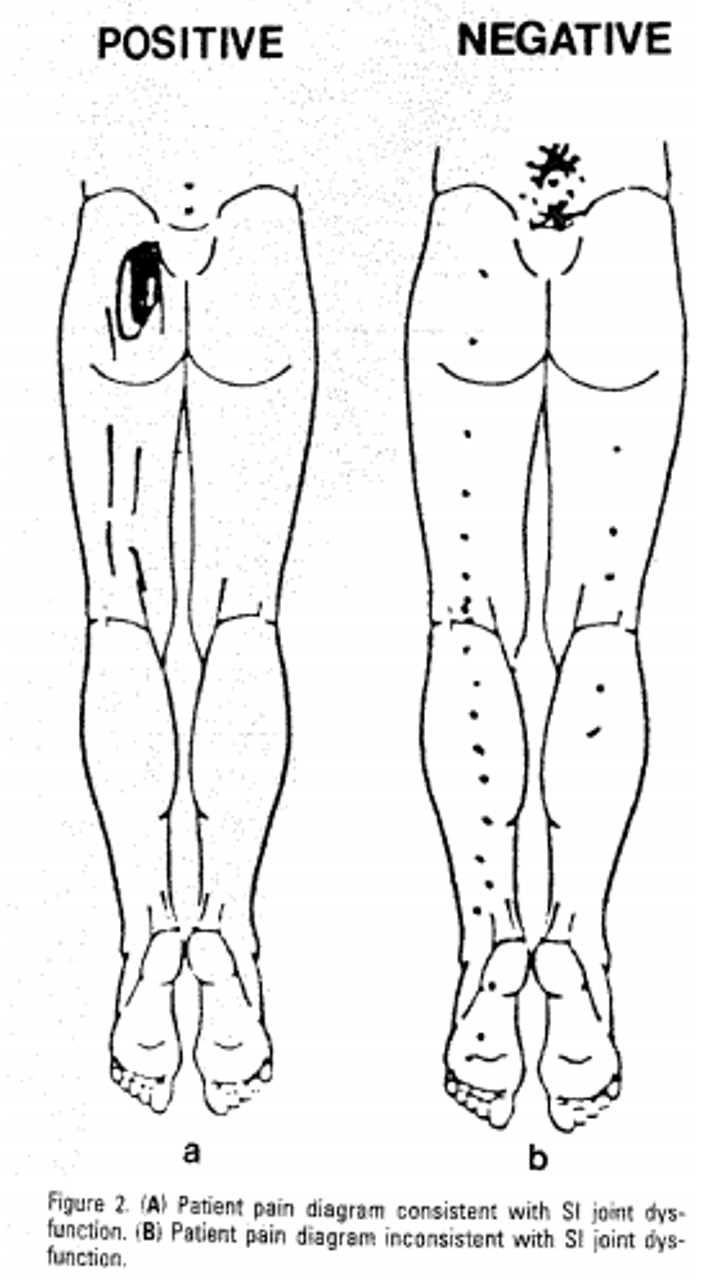
The Fortin finger sign suggests that if you’ve got pain within 1 cm of the PSIS you’re more likely to have SIJ pain (7). It’s called the Fortin finger sign because the patient would usually point towards this area with their finger. Above, you can see the difference on the pain drawing between those that responded to an SIJ block (left) versus those that didn’t respond (right) (8).
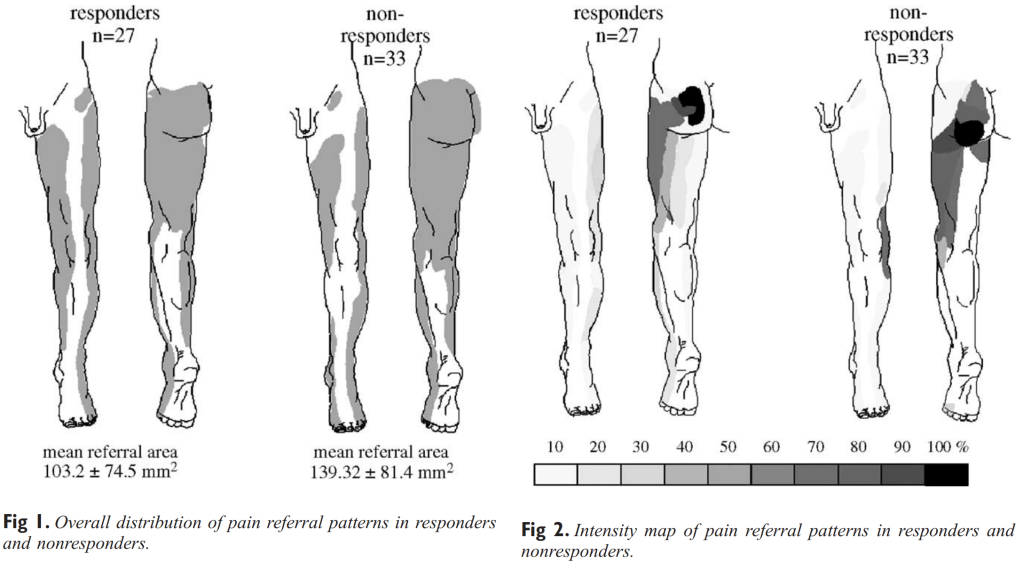
Another study from van der Wurff did the same (9). See the difference between responders and non-responders. The most obvious is that the non-responders’s pain is more inferior. Makes sense!
Maybe a bit of groin pain, but not much? I have seen some patients with a lot of groin pain, but in my experience, this is the patient with an acute, high-level pain sacroiliitis. And they had a lot of pain both in the front and the back.
Even though Fortin finger sign is a good indicator, it’s not enough to set the diagnosis. In one study only 18 out of 38 patients (48%) with this sign responded to a SIJ block. So, it can guide us in the right direction, but it’s not enough as a stand-alone sign of course.
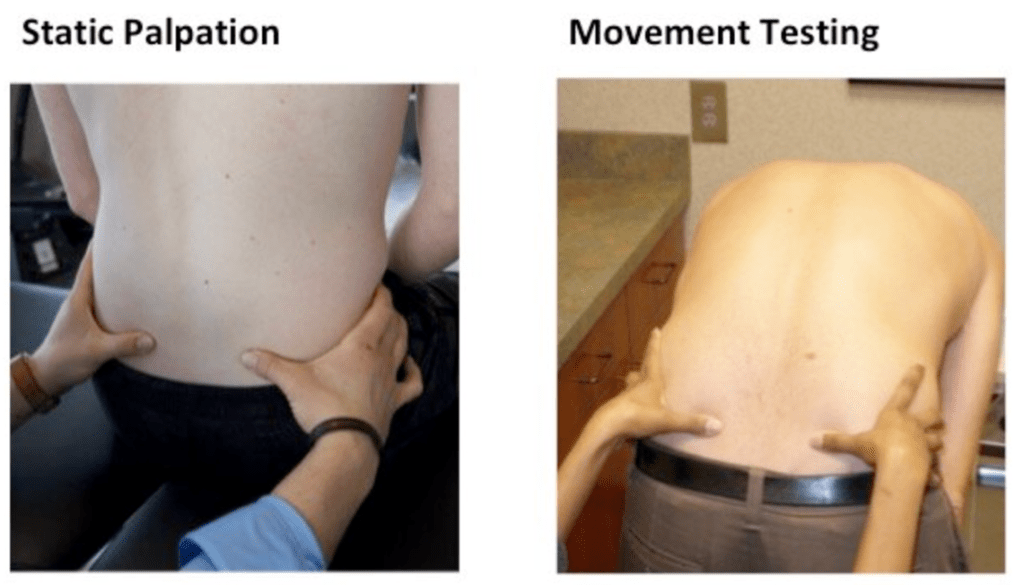
This brings us on to the next, clinical examination. What tests do we do to rule out or rule in SIJ pain? Let’s start out by talking about some myths regarding the SIJ. Of course we’re talking about the palpation and the “joint play”/motion palpation tests.
Can you feel that movement?
In my mind these myths have been busted decades ago, and I’d like to think that most people don’t believe in them, but I thought I’d include them. Because: Some people claim they can assess joint motion and asymmetry, e.g. if the ilium is rotated forward or backwards, and feel when it’s “abnormal”. Then some clinicians think that they can manipulate the sacroiliac joint “back into place”. Great sales model, eh?

First off, I have troubles understanding how you can feel a few millimetres of movement through capsule, ligaments and other structures? This shows up in studies looking at INTRA-tester reliability of motion palpation tests of the SIJ (feeling how the joint moves). Intra-tester reliability means that that the same therapists test the same patient, and tells us what they feel. Is the pelvis rotated this or that way? Is one of the joints “dysfunctional”? A systematic review and meta-analysis from 2021, looked at 15 palpation tests for SIJ (10). They could only see that the seated flexion test had moderate to intratester agreement, the other 14 were quite bad. So, if the SAME therapist can’t agree what they feel over time, what worth is the test then?
Needless to say, INTER-tester reliability is also crap (11,12). Different therapists testing the same person can’t agree at all what they feel.
Anatomical landmarks
What about the anatomical landmarks? PSIS etc? Maybe that’s easier for the therapists to find and agree on?
Unfortunately, it’s a bit of the same story: Very poor inter and intra tester reliability when they try to find the anatomical landmarks of the pelvis (13,14). Some researchers even did a study where they hid a 5 mm wedge under one of the feet, and still the therapists couldn’t figure out the asymmetry of PSIS (15). A side note, but still relevant: Do you think you’re good at finding C7 and L5? Probably not. A study showed moderate inter-tester reliability for L5 and poor reliability for C7 palpation (16). We’re all feeling different things, just like tale of the blind men and the elephant.
Back to the pelvis: A systematic review from 2016 looking palpation testing of PSIS also showed how difficult it is for people to agree, and they questioned whether these tests should be done at all (which I agree with) (17). In the article from Holmgren and Waling (13) they stated:
For clinical practise, continued use of these tests as methods for detecting asymmetry and selecting interventions is of doubtful utility
It’s normal to be asymmetric
If we therapists tested and found asymmetries, would it be abnormal? The answer is no! It’s normal to be abnormal!!
All studies looking at anatomy show normal variations of everything. Bones, muscles, nerves. Same with pelvis and spinal anatomy.
Cadaver studies shows that it is normal to have a difference in pelvic anatomical landmarks. When checking the PSIS and ASIS there was actually up to a 16 mm difference in height (18). Did you also know, almost everyone has a leg length discrepancy? In one study, they saw that 90 % had uneven leg anatomy, and the mean difference was 5 mm (19).
What about sacroiliac joint anatomy? Does it have a normal variation? This study from 2026 looked at the SIJ, and they found 8 different variants, see below (20).
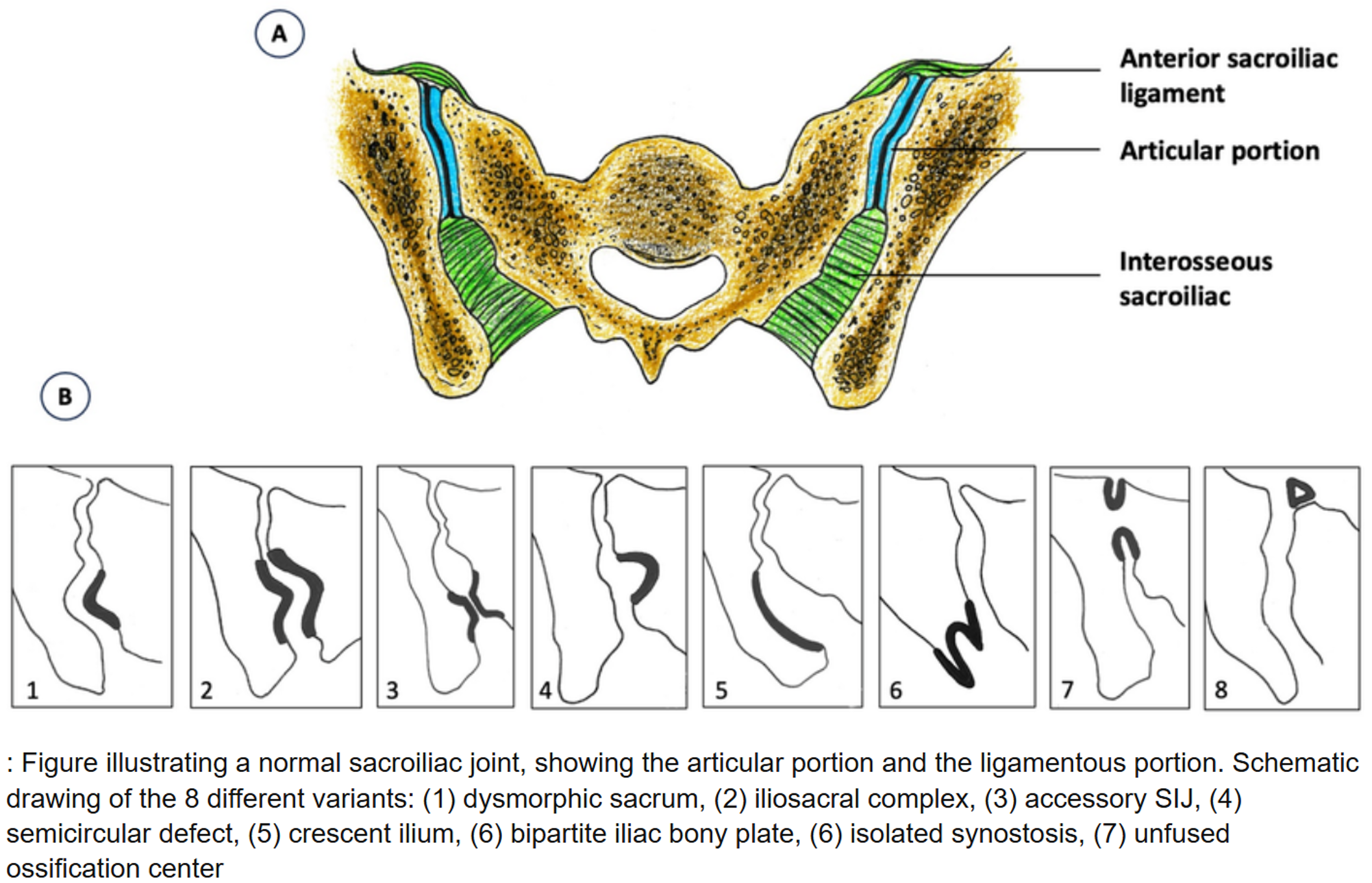
They saw a variant in 3 out of 4 people, the most common was number 4 – a semicircular defect (1 out of 4 had this), and number 2 – iliosacral complex complex (1 out of 5). Again, a proof that we’re all build different, and this is normal!
And do SIJ asymmetries and joint movement relate to pain?
And this brings us to the big question that hasn’t been asked so far? What’s the validity of these palpation and motion-palpation tests? Would the conclusion or the treatment change based on what you find? Are you testing something that is really relevant?
My thoughts so far: If you can’t agree on what you feel, and it’s normal to be asymmetrical – you don’t have a very strong case for your validity! I would say this is a case of low reliability and low validity! Shots are fired “all over the gaff”.

The thinking that the body needs to be symmetric and “normal” is part of the debunked postural-structural-biomechanical view of the body and its relation to pain (21).
Yes we have one study showed that having > 6 mm leg length discrepancy was associated with more intense back pain, but this was within a population of meat cutters and they couldn’t see this for customer service workers (22). And on the other side there are also lots of studies showing that leg length discrepancy does not matter for pain (23,24). According to a study it does not appear to be of clinical significance until it reaches about 2 cm difference! What about lumbar curve, pelvic tilt and muscle length – do these relate to back pain? Comparing groups of people with and without back pain there is no difference in their anatomy and posture (25).
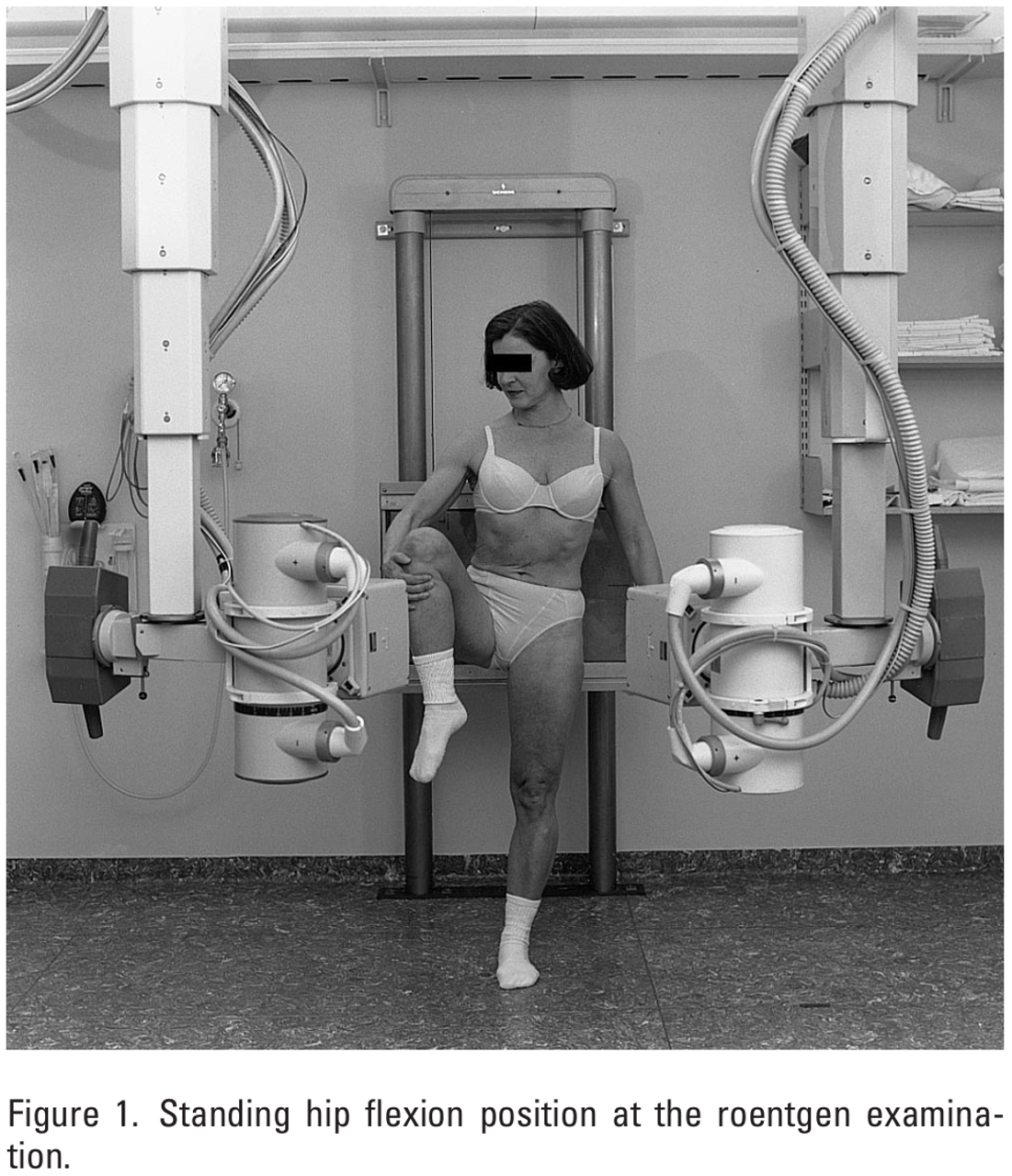
Looking specifically at the SIJ and how it moves: A painful and pain free joint does not differ in how they move! Stureson found no difference in movement between the symptomatic and asymptomatic side when they evaluated with an x-ray technique and standing hip flexion (picture below)(26).
A lot of the treatment methods are also flawed. Some therapists claim to manipulate the SIJ back into its position. And do you know what? They have actually tested if this happens or not (even though a lot of therapists, who’s business model relies on this, wouldn’t want to believe it). They did a study where they recruited patients with unilateral SIJ joint pain. The therapists felt where the “dysfunction” was and manipulated it back its place. They did an x-ray before and after. And surprise, surprise – there was no difference.
What bothers me
What is the psychological effect of being told that your pelvis is out of position/alignment, and needs to be “fixed”? It reinforces a belief that the body is fragile, and that you need others to help you recover (external locus of control). If it was me I would feel really scared and apprehensive about movement if the joints would just “pop out” easy like that. O’Sullivan and Beales talk about patients with excessive contraction and inhibition. These patients have misguided beliefs that their spine and pelvis is unstable or displaced (2). It’s quite sad.
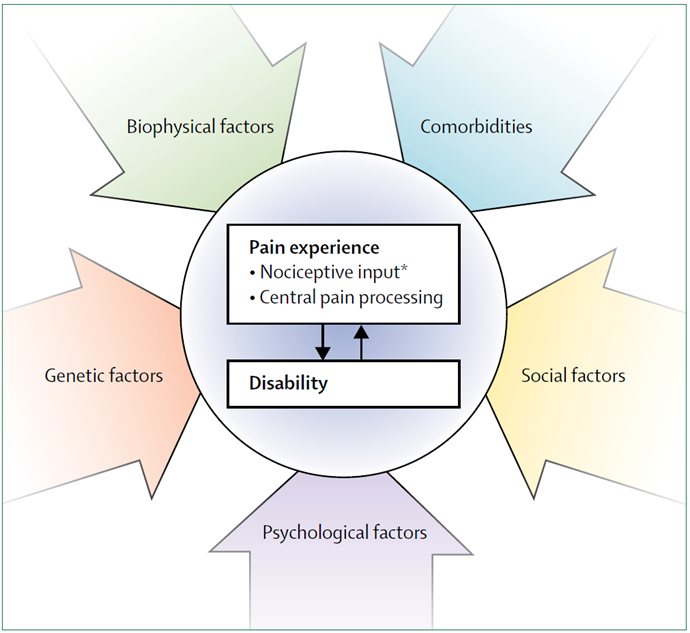
There are lots of factors that can influence pain, including SIJ pain (27). It’s so easy for therapists to point to the negative things about our patients – about what’s wrong. And very easy (and very wrong) to say that something is out of position and you can fix it. I think it’s so important to try build confidence and capacity. As Louis Gifford said we should aim for with our patients: “Thoughtless fearless movement”.
Be careful what you say to your patients, and don’t be a yellow flag.

Summary
Don’t forget about the SIJ when it comes to low back pain. More often seen with high force injuries/load, during/after pregnancy, rheumatic disease, low back pain/surgery. We can’t agree on what we feel when testing the sacroiliac joint. It would not matter if you could, because it does not matter for your pain. Other tests are be better. The body is robust, it can handles a few asymmetries here and there. If you’ve had your asymmetries the whole life your body has probably gotten used to them, and they’re just part of being you.
In the next article I will look at which tests that actually are good when you want to assess the sacroiliac joint. Later on I will talk a bit about PGP and sacroiliitis. Thanks for reading!
References
1. Booth J, Morris S. The sacroiliac joint – Victim or culprit. Best Pract Res Clin Rheumatol. 2019 Feb;33(1):88–101. doi:10.1016/j.berh.2019.01.016 PubMed PMID: 31431277.
2. McCormick ZL, Hurley RW, Anitescu M, Bhaskar A, Bhatia A, Cassidy RC, et al. Consensus practice guidelines on sacroiliac joint complex pain from a multispecialty, international working group. Pain Med. 2025 Dec 1;26(12):817–917. doi:10.1093/pm/pnaf129 PubMed PMID: 41318933; PubMed Central PMCID: PMC12681192.
3. Goode A, Hegedus EJ, Sizer P, Brismee JM, Linberg A, Cook CE. Three-dimensional movements of the sacroiliac joint: a systematic review of the literature and assessment of clinical utility. J Man Manip Ther. 2008;16(1):25–38. doi:10.1179/106698108790818639 PubMed PMID: 19119382; PubMed Central PMCID: PMC2565072.
4. Kibsgård T. Radiostereometric analysis of sacroiliac joint movement and outcomes of pelvic joint fusion. Acta Orthopaedica. 2015 Feb 28;86:S1–40. doi:10.3109/17453674.2015.1022707
5. Fagevik Olsén M, Körnung P, Kallin S, Elden H, Kjellby Wendt G, Gutke A. Validation of self-administered tests for screening for chronic pregnancy-related pelvic girdle pain. BMC Musculoskelet Disord. 2021 Mar 1;22(1):237. doi:10.1186/s12891-021-04103-0 PubMed PMID: 33648489; PubMed Central PMCID: PMC7923664.
6. McCrum C, Chambers H. Masterclass- Axial and peripheral Spondyloarthritis: Screening, suspicion and referral in musculoskeletal clinical practice. Musculoskeletal Science and Practice. 2026 Apr 1;82:103474. doi:10.1016/j.msksp.2025.103474
7. Fortin JD, Falco FJ. The Fortin finger test: an indicator of sacroiliac pain. Am J Orthop (Belle Mead NJ). 1997 Jul;26(7):477–80. PubMed PMID: 9247654.
8. Fortin JD, Aprill CN, Ponthieux B, Pier J. Sacroiliac joint: pain referral maps upon applying a new injection/arthrography technique. Part II: Clinical evaluation. Spine (Phila Pa 1976). 1994 Jul 1;19(13):1483–9. PubMed PMID: 7939979.
9. van der Wurff P, Buijs EJ, Groen GJ. Intensity mapping of pain referral areas in sacroiliac joint pain patients. J Manipulative Physiol Ther. 2006 Apr;29(3):190–5. doi:10.1016/j.jmpt.2006.01.007 PubMed PMID: 16584942.
10. Ribeiro RP, Guerrero FG, Camargo EN, Beraldo LM, Candotti CT. Validity and Reliability of Palpatory Clinical Tests of Sacroiliac Joint Mobility: A Systematic Review and Meta-analysis. J Manipulative Physiol Ther. 2021 May;44(4):307–18. doi:10.1016/j.jmpt.2021.01.001 PubMed PMID: 33896601.
11. Potter NA, Rothstein JM. Intertester Reliability for Selected Clinical Tests of the Sacroiliac Joint. Phys Ther. 1985 Nov 1;65(11):1671–5. doi:10.1093/ptj/65.11.1671
12. Holmgren U, Waling K. Inter-examiner reliability of four static palpation tests used for assessing pelvic dysfunction. Man Ther. 2008 Feb;13(1):50–6. doi:10.1016/j.math.2006.09.009 PubMed PMID: 17210266.
13. Holmgren U, Waling K. Inter-examiner reliability of four static palpation tests used for assessing pelvic dysfunction. Man Ther. 2008 Feb;13(1):50–6. doi:10.1016/j.math.2006.09.009 PubMed PMID: 17210266.
14. Robinson HS, Brox JI, Robinson R, Bjelland E, Solem S, Telje T. The reliability of selected motion- and pain provocation tests for the sacroiliac joint. Man Ther. 2007 Feb;12(1):72–9. doi:10.1016/j.math.2005.09.004 PubMed PMID: 16843031.
15. Sutton C, Nono L, Johnston RG, Thomson OP. The effects of experience on the inter-reliability of osteopaths to detect changes in posterior superior iliac spine levels using a hidden heel wedge. J Bodyw Mov Ther. 2013 Apr;17(2):143–50. doi:10.1016/j.jbmt.2012.07.005 PubMed PMID: 23561859.
16. Robinson R, Robinson HS, Bjørke G, Kvale A. Reliability and validity of a palpation technique for identifying the spinous processes of C7 and L5. Manual Therapy. 2009 Aug;14(4):409–14. doi:10.1016/j.math.2008.06.002
17. Cooperstein R, Hickey M. The reliability of palpating the posterior superior iliac spine: a systematic review. J Can Chiropr Assoc. 2016 Mar;60(1):36–46. PubMed PMID: 27069265; PubMed Central PMCID: PMC4807681.
18. Preece SJ, Willan P, Nester CJ, Graham-Smith P, Herrington L, Bowker P. Variation in Pelvic Morphology May Prevent the Identification of Anterior Pelvic Tilt. J Man Manip Ther. 2008;16(2):113–7. doi:10.1179/106698108790818459 PubMed PMID: 19119397; PubMed Central PMCID: PMC2565125.
19. Knutson GA. Anatomic and functional leg-length inequality: A review and recommendation for clinical decision-making. Part I, anatomic leg-length inequality: prevalence, magnitude, effects and clinical significance. Chiropr Osteopat. 2005 Jul 20;13:11. doi:10.1186/1746-1340-13-11 PubMed PMID: 16026625; PubMed Central PMCID: PMC1232860.
20. Le Baron M, David G, Ward BA, Mauffrey C. Sacroiliac joint variants are common and gender-specific but do not predict fracture pattern in pelvic ring injuries. Eur J Orthop Surg Traumatol. 2026 Feb 19;36(1):112. doi:10.1007/s00590-026-04682-5 PubMed PMID: 41711917.
21. Lederman E. The fall of the postural-structural-biomechanical model in manual and physical therapies: exemplified by lower back pain. J Bodyw Mov Ther. 2011 Apr;15(2):131–8. doi:10.1016/j.jbmt.2011.01.011 PubMed PMID: 21419349.
22. Rannisto S, Okuloff A, Uitti J, Paananen M, Rannisto PH, Malmivaara A, et al. Leg-length discrepancy is associated with low back pain among those who must stand while working. BMC Musculoskelet Disord. 2015 May 7;16:110. doi:10.1186/s12891-015-0571-9 PubMed PMID: 25943907; PubMed Central PMCID: PMC4433073.
23. Helliwell M. Leg length inequality and low back pain. Practitioner. 1985 May;229(1403):483–5. PubMed PMID: 3160015.
24. Grundy PF, Roberts CJ. DOES UNEQUAL LEG LENGTH CAUSE BACK PAIN?: A Case-control Study. The Lancet. 1984 Aug 4;Originally published as Volume 2, Issue 8397324(8397):256–8. doi:10.1016/S0140-6736(84)90300-3
25. Nourbakhsh MR, Arab AM. Relationship between mechanical factors and incidence of low back pain. J Orthop Sports Phys Ther. 2002 Sep;32(9):447–60. doi:10.2519/jospt.2002.32.9.447 PubMed PMID: 12322811.
26. Sturesson B, Uden A, Vleeming A. A radiostereometric analysis of movements of the sacroiliac joints during the standing hip flexion test. Spine (Phila Pa 1976). 2000 Feb 1;25(3):364–8. doi:10.1097/00007632-200002010-00018 PubMed PMID: 10703111.
27. Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet. 2018 09;391(10137):2356–67. doi:10.1016/S0140-6736(18)30480-X PubMed PMID: 29573870.
