Further down is an overview I’ve created to help differentiate between fibular neuropathy (peroneal neuropathy) and L5 radiculopathy in clinical practice.
First, a clarification: yes, I’ve always thought “peroneus” was the best term to use, but I was made aware that “fibularis” is preferred. This is because “peroneal” can be confused with “perineal,” which relates to the perineum (for those who didn’t know, the perineum is the area between the anus and the genitals). Thanks for the clarification, Magnus!
Here’s the “official answer” if you want to nerd out on anatomical terminology (I’m guessing very few do) (1):
Enough talk—here’s the overview:
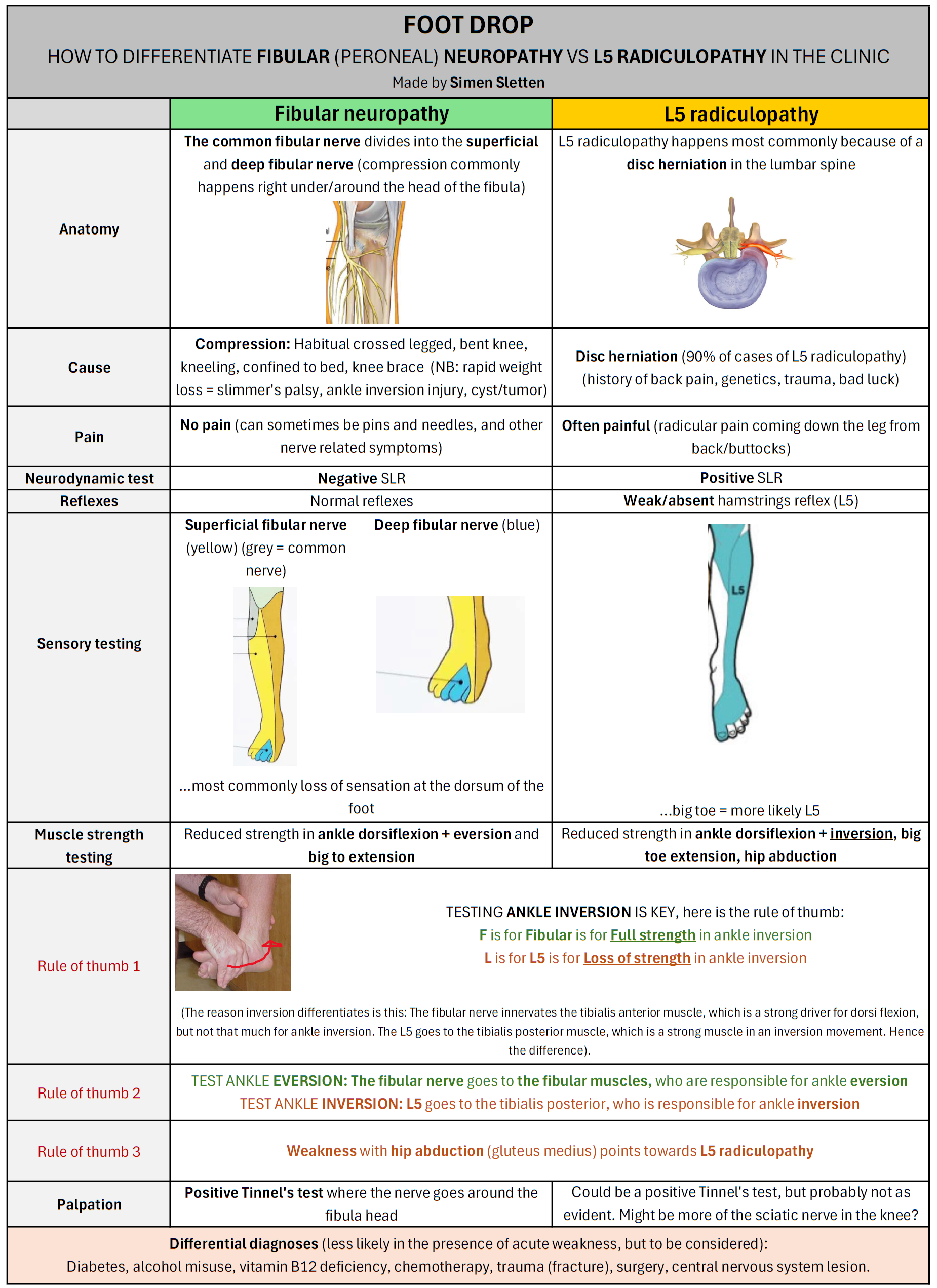
The most important question you can ask in the subjective to differentiate the two is whether there is pain—yes or no. If there is no pain or other neurological symptoms, it is almost always fibular neuropathy (2).
On examination, the key is to test ankle inversion. In fibular neuropathy, inversion strength will be preserved, whereas in L5 radiculopathy there will be weakness. This is because the fibular nerve innervates the tibialis anterior (important for dorsiflexion, but not as important for inversion), while L5 innervates the tibialis posterior (which is the primary muscle responsible for ankle inversion) (3,4).
Fibular neuropathy most often occurs in people who get a compression of the nerve over time—for example, by sitting with their legs crossed or squatting for prolonged periods. It is, of course, important to be aware of differential diagnoses such as diabetes, alcohol misuse, vitamin B12 deficiency, and central or peripheral nerve disorders (2).
One of the more interesting findings when I reviewed the literature was “slimmer’s palsy/paralysis,” where rapid weight loss increases the risk of fibular neuropathy. This is particularly relevant in these “Ozempic times” (5).
Treatment?
These are recommendations according to Stevens et al. (2):
- Refer immediately to a neurologist if there is acute bilateral foot drop, or within one week if there is unilateral foot drop with fasciculations and widespread neuropathy
- Refer urgently to a surgeon if you suspect acute compartment syndrome
- If it is a “normal” fibular neuropathy caused by compression around the knee, advise the patient to avoid sitting with legs crossed, prolonged squatting, and kneeling. Strength will usually return within 2–3 months
- Recommend flat, supportive footwear to reduce the risk of ankle sprains. Use an orthosis if there is significant weakness
- Physiotherapy and exercise
- Follow up within two months, and refer to a neurologist if there is no improvement
References
1. Federative international programme on anatomical terminologies, editor. Terminologia anatomica: international anatomical terminology. 2nd ed. Stuttgart: Thieme; 2011.
2. Stevens F, Weerkamp NJ, Cals JWL. Foot drop [Internet]. 2015 Apr 27. doi:10.1136/bmj.h1736
3. Reife MD, Coulis CM. Peroneal neuropathy misdiagnosed as L5 radiculopathy: a case report. Chiropr Man Therap. 2013 Apr 22;21:12. doi:10.1186/2045-709X-21-12 PubMed PMID: 23618508; PubMed Central PMCID: PMC3662609.
4. Fortier LM, Markel M, Thomas BG, Sherman WF, Thomas BH, Kaye AD. An Update on Peroneal Nerve Entrapment and Neuropathy. Orthop Rev (Pavia). 2021;13(2):24937. doi:10.52965/001c.24937 PubMed PMID: 34745471; PubMed Central PMCID: PMC8567814.
5. Cucu LE, Popescu G, Maștaleru A, Ignat EB, Grosu C, Bîrsanu L, et al. Common Peroneal Nerve Paralysis Following Rapid Weight Loss-A Case Report and Literature Review. Nutrients. 2025 May 24;17(11):1782. doi:10.3390/nu17111782 PubMed PMID: 40507050; PubMed Central PMCID: PMC12157737.
