
I want to say in advance, this is a long article. Sorry!
There, I said it. Let’s begin…
First things first
If you ONLY have pain in the lower back, meaning low back pain WITHOUT leg pain — you should not have surgery (with a very, very, very few exceptions?).
Surgery will likely do more harm than good!
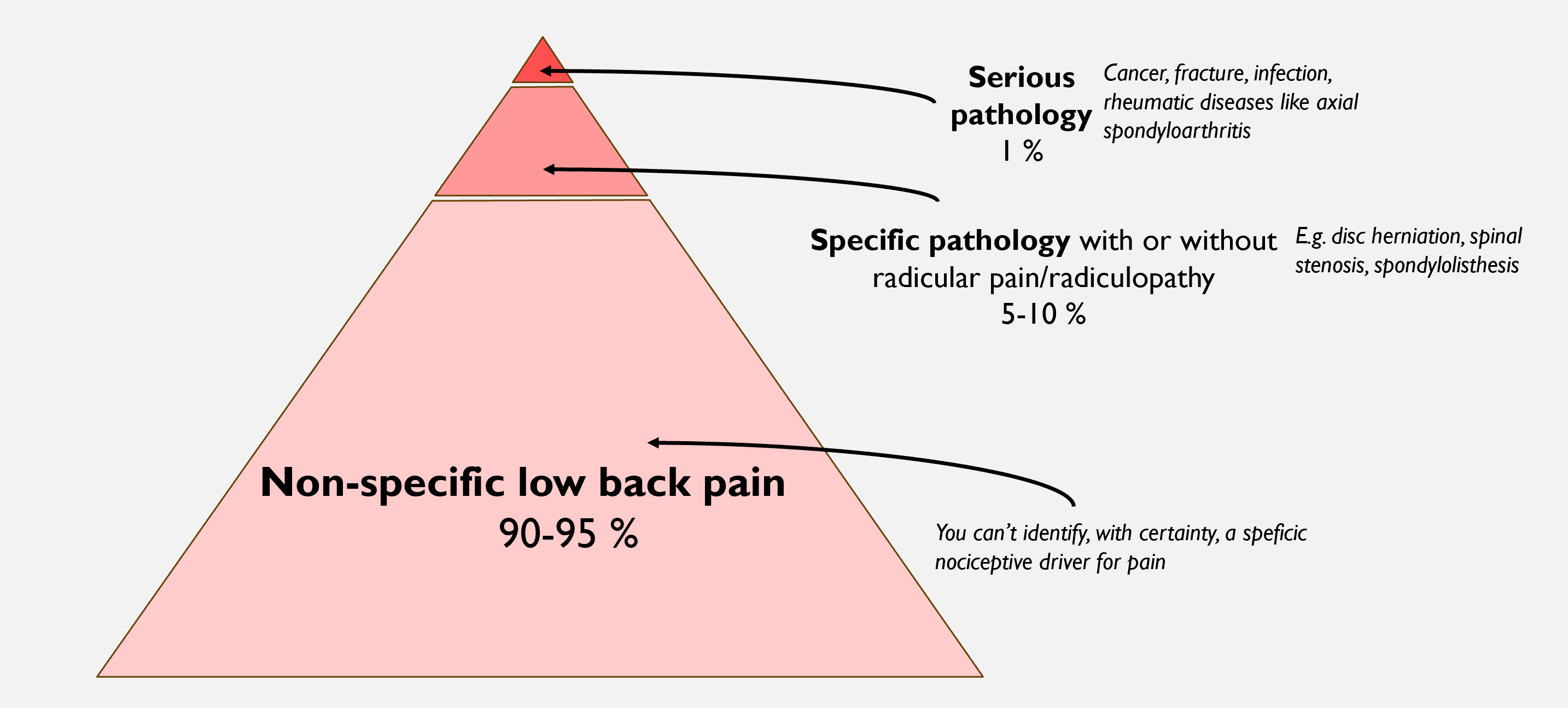
Approximately 90–95% of people with low back pain have what we call “ordinary low back pain”, or non-specific low back pain) (1) (Although several clinicians and researchers argue that “non-specific low back pain” is a poor term, and that more specific diagnoses can often be made, such as disc-related or facet joint pain. More about this later?).
Among those who consult a GP or physiotherapist because of low back pain, only about 5–10% have sciatica (when I use the term sciatica here, I mean nerve-related leg pain, also known as radicular pain) (2,3).
Of these, even fewer have actually have a lumbar disc herniation with sciatica. The lifetime prevalence of disc herniation with sciatica is estimated to be 5.3% in men and 3.7% in women (4,5).
Most patients do not need surgery
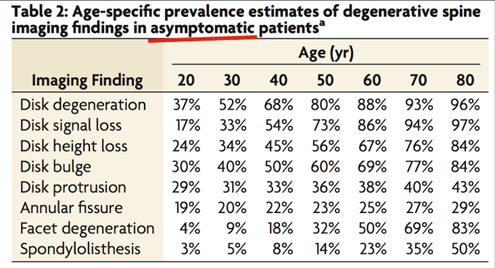
Even if you have a disc herniation with sciatica, the probability that you will need surgery is very small. Around 90–95% of patients respond well to conservative treatment (6). This means that only about 5–10% of those with a disc herniation are candidates for surgery. Keep in mind that this likely refers to 5–10% of those with a symptomatic disc herniation. We know that many people have disc herniations WITHOUT any back or leg pain. The literature suggests that overall, only about 2% of patients with back complaints undergo surgery for disc herniation (6). In other words, the vast majority recover on their own, or are able to manage their symptoms without surgery.
So those are the basic premises.
Once again: very few patients actually need surgery.
In this article, I will try to clarify this topic a bit further.
Three groups
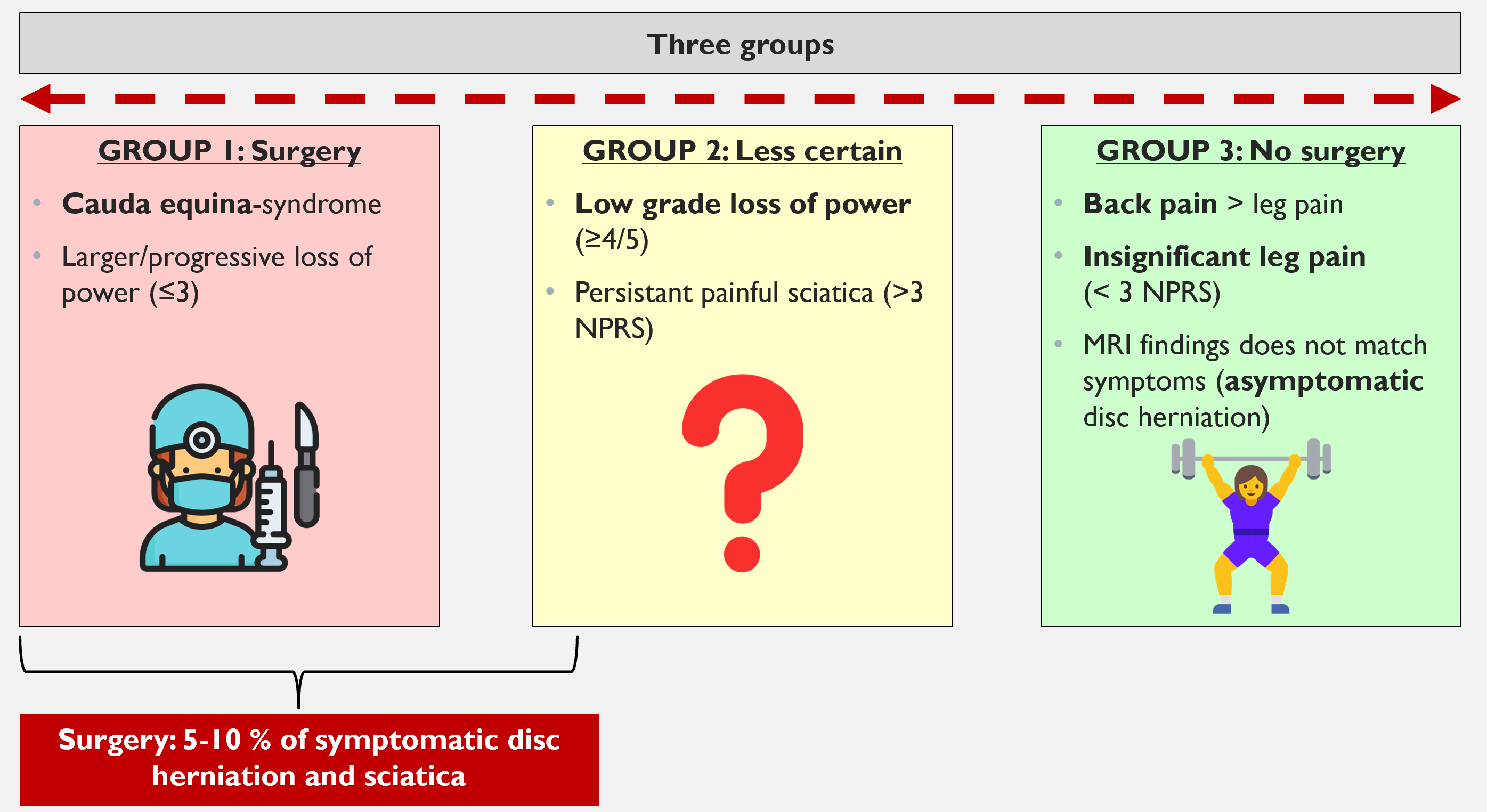
When discussing lumbar disc herniation, the neurologist and researcher Henrik Weber proposed that patients can be divided into three categories:
- Group 1: Patients who clearly need surgical intervention
- Group 2: Patients for whom it is uncertain whether surgery is necessary
- Group 3: Patients who do not have a good indication for surgery
In simple terms, the situation looks like this—although we will go into more detail.
Focus of this article
In this article, I will mainly discuss Group 2, the patients for whom it is uncertain whether surgery is necessary or not.
But first, I will briefly mention the two other groups.
A historical (Norwegian) side note
Henrik Weber was a physician and researcher who became a pioneer in research on disc herniation and sciatica. In the 1970s, he conducted a randomized controlled trial that followed patients for ten years, comparing surgical treatment with conservative treatment (7). Like any study, it has both strengths and weaknesses. Nevertheless, it remains one of only a few major studies in this field with very long-term follow-up (we will return to it later. And, of course, it is particularly cool that he was Norwegian.
Let’s return to the three groups:
Group 1: Patients Who Clearly Should Have Surgery
The first group — those who clearly need surgical intervention — was discussed in the article
“Lumbar Disc Herniation – Who Should Be Referred to Hospital and MRI?”
The summary is as follows:
You should make an emergency referral in cases of cauda equina syndrome and significant or progressive motor weakness. Be alert to other red flags. Call the on-call physician to discuss the case before admitting the patient if appropriate (at least in Norway). For those who do not require emergency care, it is uncertain how beneficial early MRI and early surgical assessment actually are. Much of the literature suggests that early MRI should often be avoided, and in some cases MRI may not be necessary at all.
When urgent referral is necessary
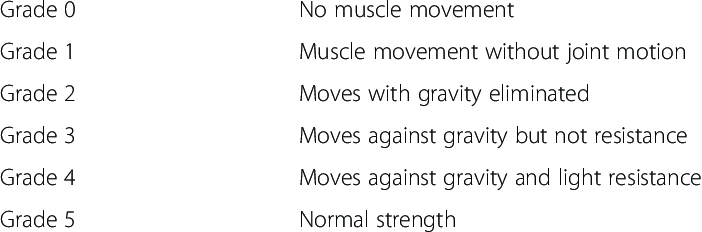
In other words, if there are signs of disc herniation with cauda equina syndrome or significant/progressive motor deficit (grade 3 strength or worse), the patient should be referred for urgent hospital assessment. There is consensus that surgery is the preferred treatment for these patients (9). Many are operated on quickly because the nerves may suffer permanent damage. Some hospitals recommend admission within 72 hours after a major motor deficit, and possibly surgery within one week.
Interestingly, there is a paradox here. Patients with larger disc herniations often have a better prognosis— “The bigger the bulge, the better.” I have personally seen many patients with foot drop who later regained full muscle strength. So the situation is not entirely black and white. Another surgeon I talked to said he you also could wait 4-6 weeks, at a maximum, before doing surgery on a patient with radiculopathy. That way you could see if the patient showed signs of improving or not, and base your decision off that.
Nevertheless, good clinical practice is to refer these patients to hospital, so they receive rapid and appropriate assessment.
Group 3: Those who should not have surgery
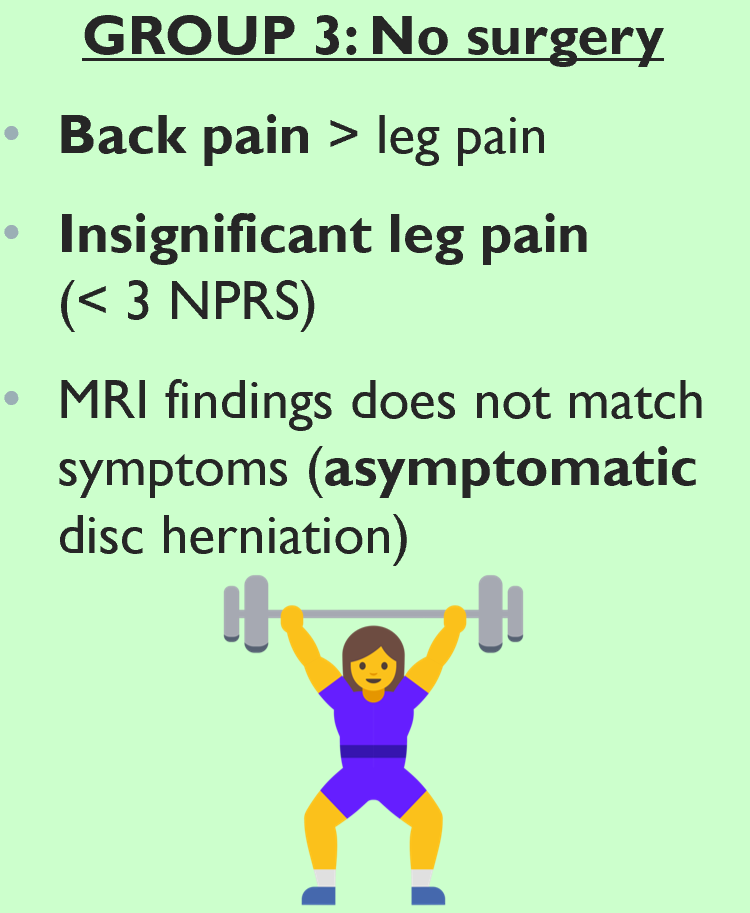
It is important to understand that the purpose of surgery is to treat the leg pain — not back pain. If you have a disc herniation and only back pain, you should not undergo surgery. We know that disc herniations are common even in people without pain, so the back pain may not even be caused by the herniation in the first place.
We also have studies showing that patients with milder symptoms tend to have worse outcomes following surgery.
Patients with low levels of leg pain (< 3 on the pain scale) have a high risk of becoming worse after surgery (10). A similar pattern is seen in spinal stenosis: patients who undergo surgery with only minor leg pain may actually experience increased leg pain afterward (11). Likewise, patients who have more back pain than leg pain tend to have poorer surgical outcomes (12)
Take a moment to reflect on this:
if leg pain is minimal, and/or back pain is more dominant than leg pain, surgery is unlikely to be beneficial.
Another critical point is diagnostic accuracy.
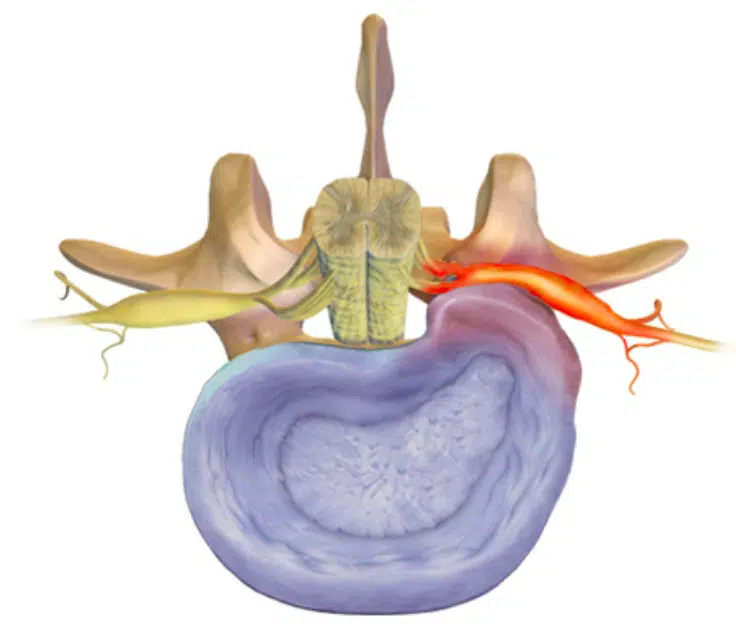
You can have a disc herniation and leg pain without the pain being radicular. Other structures can also produce leg pain — known as somatic referred pain. For example, the hip joint, sacroiliac joint, and facet joints can generate nociceptive input that leads to somatically referred pain into the leg (see image). As I’ve said many times, the patient history and clinical examination are essential.
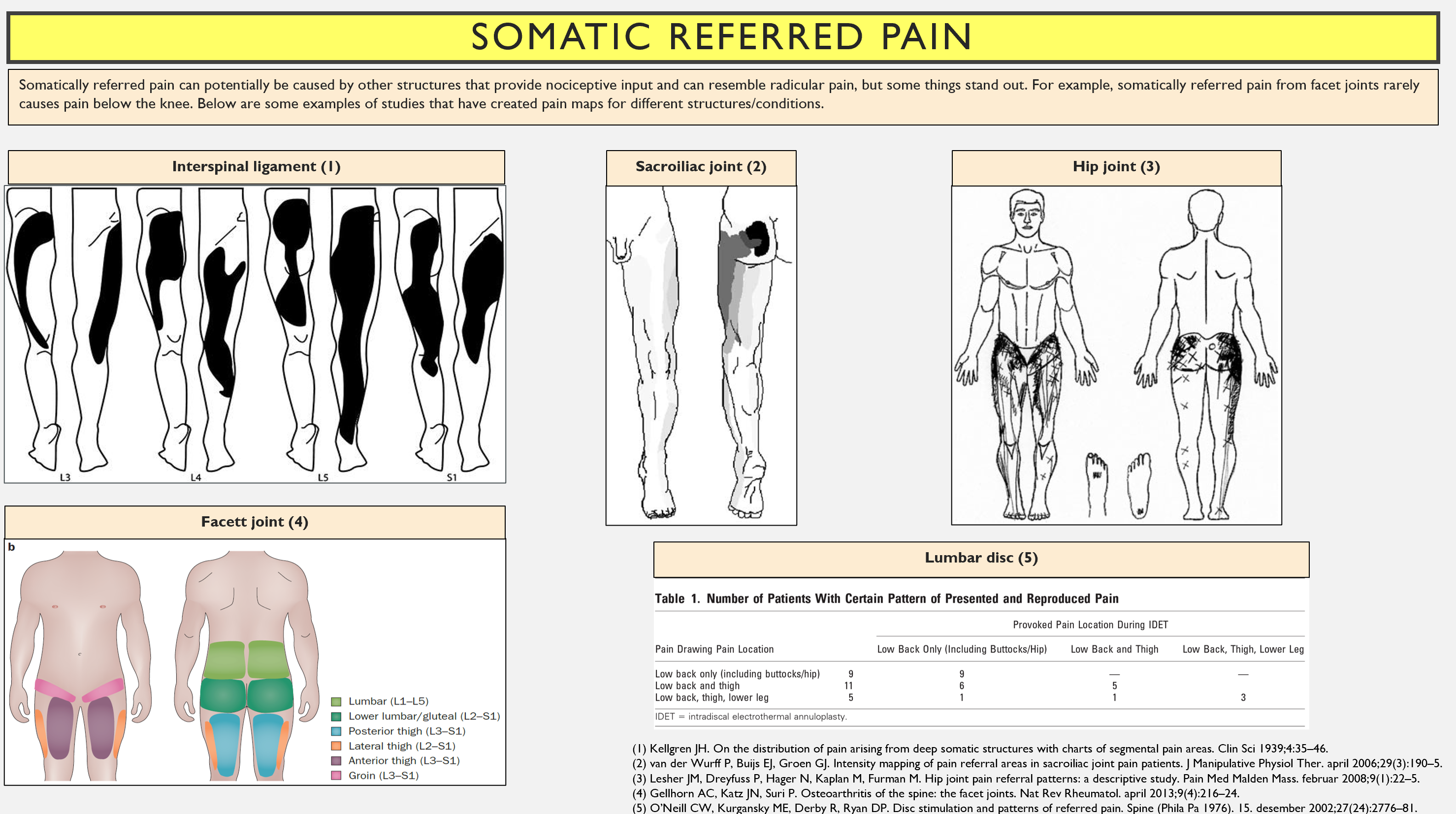
For more information, read my article here: https://thescandiphysio.com/2024/05/20/are-disc-herniations-painful/
Group 2: The Grey zone – When It Is Unclear Whether Surgery Is Indicated
The most challenging group consists of the so-called “grey zone” patients—those with painful sciatica but without significant motor deficit (≥ grade 4) or other major neurological findings. Who among these should undergo surgery?
Let’s start with the short answer:
In general, surgery appears to provide faster pain relief, but in the long term, there is no meaningful difference between surgical and conservative treatment (13–15). Surgery also carries a risk of complications and adverse events (16).
To reiterate: this applies to patients with painful sciatica without major motor deficit. Patients with significant weakness or cauda equina syndrome are not part of this category.
A figure that summarizes how radicular pain behaves over time can be found in Olaf Fjeld’s PhD thesis. Pain is typically high in the early phase, but after 6–12 weeks, it often decreases substantially. One year after treatment, average leg pain is generally low (NPRS ~2.5/10), regardless of whether the patient had surgery or not (9).
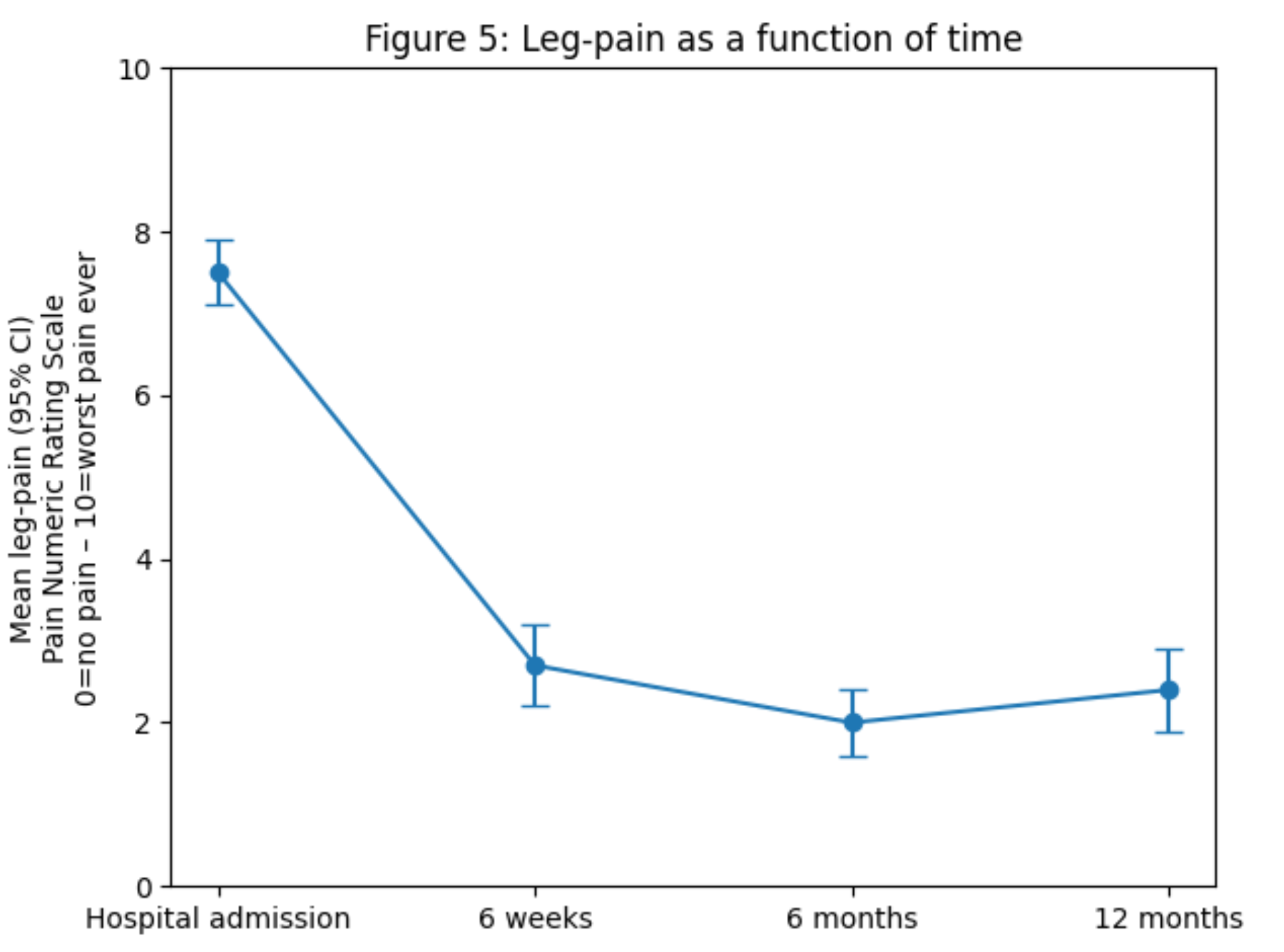
Patients who undergo surgery often start with more severe pain and tend to experience a steeper reduction in symptoms during the first 6–12 weeks, but this advantage diminishes over time (9).
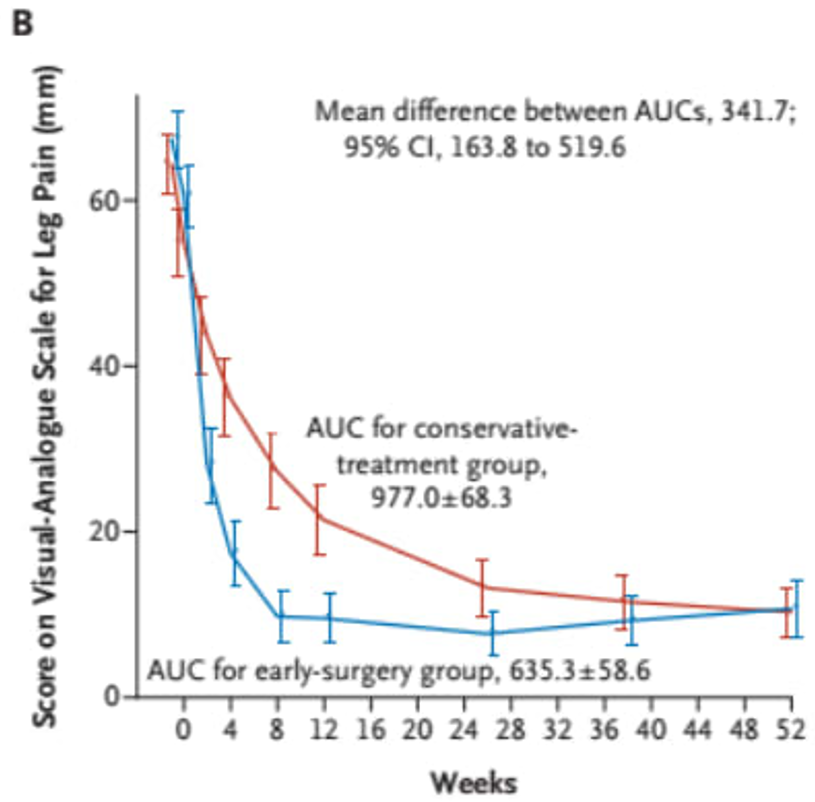
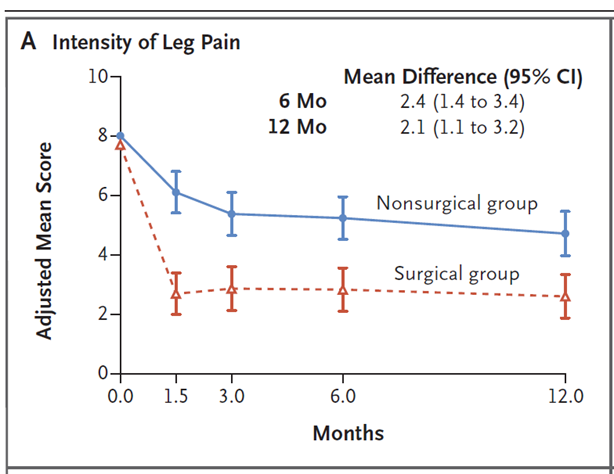
Below is an example of a study clearly showing that patients who undergo surgery experience a faster reduction in leg pain, but that the difference evens out over time. The study compared early surgery (blue line) with conservative treatment (red line). The Y-axis represents leg pain. It is clear that those who undergo surgery achieve faster pain relief, but that the difference evens out after one year. This pattern is also maintained after two years (15).(15).
In the disc herniation field, there are three major long-term studies comparing surgery and conservative treatment, based on my understanding (7,17,18).
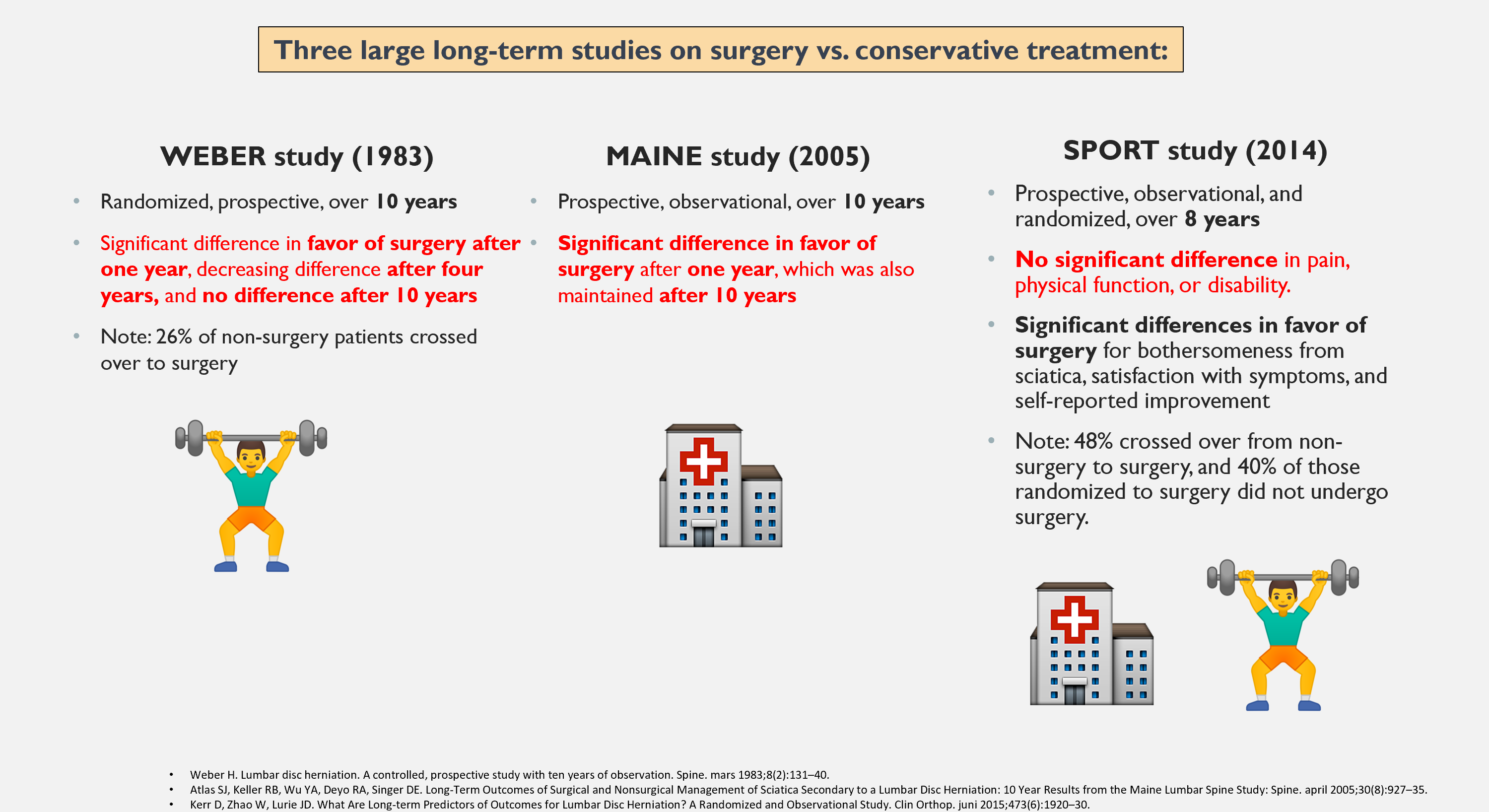
First, our Norwegian colleague Henrik Weber and his ten-year study. He found that surgery gave better results after one and four years, but no difference after ten years (7). In the Maine/Atlas study, there was a significant difference in favor of surgery, which persisted after ten years (17). The SPORT study showed mixed findings. There were no significant differences in pain and function, but there were differences in self-reported improvement and how bothersome the sciatica symptoms were (18).
A major problem with many of these studies is the cross-over effect — meaning patients randomized to one treatment switched to another. In the latter case, in the SPORT study, half of those who were supposed to receive conservative treatment ended up having surgery anyway, and 40% of those who were randomised to surgery were not operated on (18).
Overall, when it comes to disc herniation and sciatica, it is seen that 26–54% of those who are randomised to conservative treatment end up having surgery anyway. In one article, it is therefore stated that randomised controlled trials (RCTs) in reality compare early surgery with conservative treatment and delayed surgery. Researchers also question whether patients who voluntarily participate in an RCT comparing surgery and conservative treatment are representative of real-world clinical patients (14).
A prospective study by Gugliotta et al. attempted to eliminate the cross-over effect by conducting an observational study and analyzing it to resemble an RCT.
The results did not show much new.
The surgery group felt better after six weeks, but the effect disappeared after three months, and there was no difference after one and two years (14).
So, if there is no long-term difference, is there any point in operating, or should one refrain? Studies look at averages. Could there be subgroups who benefit more from surgery?
Timing and Surgery
Olaf Fjeld writes that there is general consensus that patients with pronounced painful sciatica beyond 8–12 weeks of conservative treatment should be offered surgery (9).
This is important: In his PhD, it was found that how much leg pain you have after six weeks is a predictor of how much leg pain you have after 12 months (9).
He therefore argues for increasing treatment efforts around 6–12 weeks — reassessing surgery, adjusting analgesics, scheduling follow-ups (9). Perhaps surgery should be more strongly considered after 8–12 weeks if there is no improvement.
We unfortunately do not know whether increased effort for this group leads to better outcomes. We also know that most studies show no difference after one year. As long as the pain is manageable, it may therefore be reasonable to wait and see. In some countries, including England, no one in this group is operated on before six weeks have passed. They use corticosteroid injections, among other things, to relieve pain while time passes.
The amount of leg pain at six weeks predicts the amount of leg pain at 12 months.
Another study examined when to consider follow-up MRI and possibly surgery for disc herniation and sciatica. Around two-thirds of all disc herniations resorb. The authors recommend reassessment with MRI and possible surgery at 4 and 10.5 months after symptom onset (19).
For some, it may be wise to have earlier surgery instead of “suffering through” weeks and months. I have had patients say: “Had I known how this would turn out, I would have had surgery earlier.”
Summary – Follow-up MRI/Surgery
It may therefore be wise to schedule a follow-up consultation six weeks after onset of symptoms – as a minimum, although most should be offered closer follow-up in the acute phase, because it can be really painful! I see patients every week in the first phase.
If pain is still significant after six weeks, surgery may be more strongly considered. If pain is manageable after six weeks, one can wait and possibly consider repeat MRI and surgery at 4 and 10.5 months.
If there is no change in the size of the herniation, surgery may be more strongly considered (but remember, herniation size is not necessarily correlated with symptoms. Often it is the chemical irritation in the early phase that causes pain more than the compression itself — comparable to a bee sting). Luis Gifford describes radicular pain as maladaptive. It is merely irritation/compression of a very small area of the body that produces a tremendous amount of pain. He also suggests that sciatica can be viewed as phantom pain — without the amputation (20).
Studies Do Not Examine Patients with Long-Standing Pain – What About Them?
In studies on disc herniation surgery, the focus is usually on early surgery compared with conservative treatment. But what about those who have had sciatica for a long time? Should they “endure” an even longer period too look for improvements, or should they be considered for surgery (21)?
A 2020 study examined patients who had sciatica for 4–12 months. They have had sciatica for a while, and are still suffering. They were randomized to continued conservative treatment or surgery. The surgical group had less pain after six months (this also appears to apply at 12 months, but for some reason this was not included in the conclusion — perhaps due to too many dropouts?) (22).
It may therefore appear that those with persistent sciatica can still benefit from surgery. I see this as somewhat an extension of the 6-week rule discussed earlier (23). However, we still cannot determine who should undergo early surgery, or how long one can maximally wait and still benefit. And remember, this is only one study, and it has some limitations (including missing data from 20% of participants) (22).
I also believe one reason for the strong effect was the high pain intensity (NPRS 8/10).
Patients with severe symptoms benefit most from surgery, whereas those with mild symptoms have less potential for improvement and greater risk of worsening. As previously stated, patients with leg pain NPRS 3 or lower have a high risk of worsening (10). If you only have occasional radiating pain and it is not particularly bothersome, you should therefore not undergo surgery.
This is also seen in clinical practice, in this case from a study of patients at Ullevål Hospital, when comparing the two groups – patients who underwent surgery had significantly more leg pain than those treated conservatively (around a 2-point difference on the NPRS) (23).
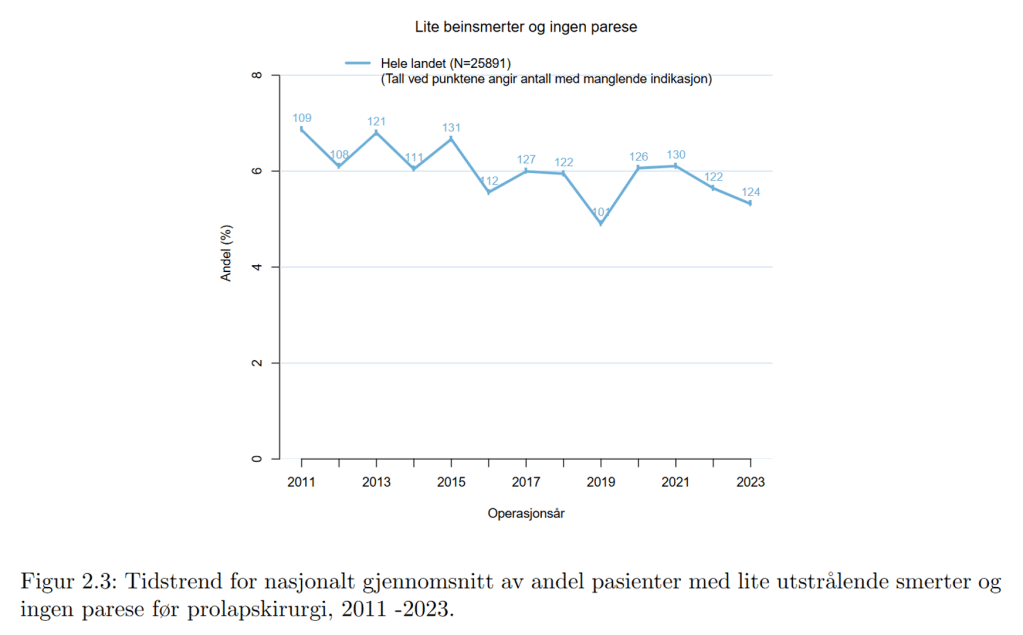
In Norway, the proportion of patients who undergo surgery without a strong indication is around 5–7%, see the figure below (patients with more severe paresis/paralysis are excluded from this calculation). This number needs to be reduced.
How Long Should One Maximum Wait Before Surgery?
The previous study showed benefit up to one year, but what do other studies show?
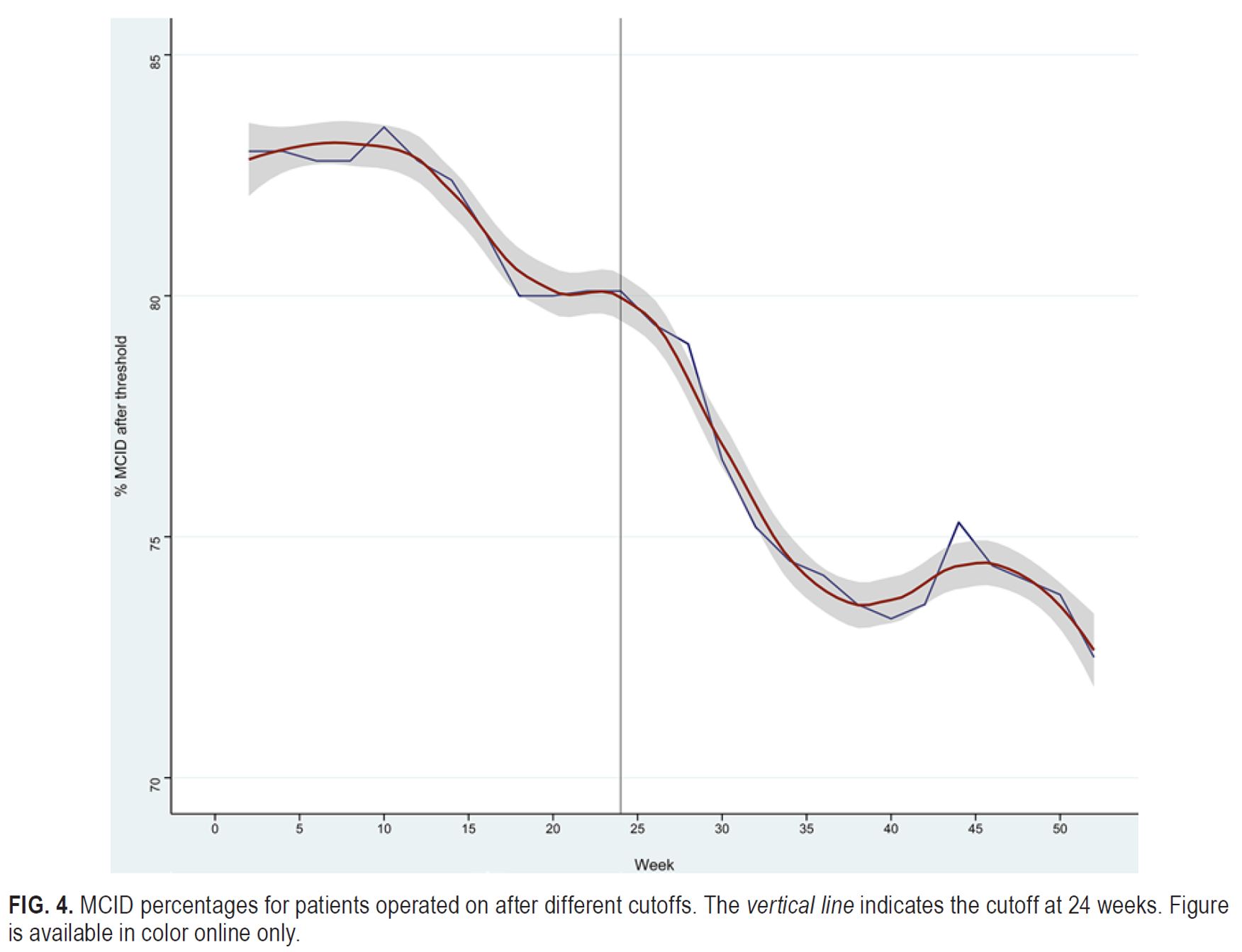
Several sources suggest operating before six months (24). Siccoli et al. examined the minimal clinically important difference (MCID), defined as a 30% improvement in leg pain from baseline. They then investigated how long this improvement persisted before declining in the research data. Results began to worsen after six months (see image) (25).
An analysis of SPORT data confirms this finding, showing that patients with symptoms lasting more than six months had poorer outcomes — both surgical and conservative (26).
Other sources suggest one can wait up to one year. Norwegian national guidelines from 2007 state that preferably no more than one year with significant leg pain should pass before surgery (27). Data from the Norwegian Registry for Spine Surgery support this, showing that patients operated for disc herniation with leg pain lasting more than one year have poorer prognosis (10).
According to Norwegian register data, approximately half of those undergoing surgery have had pain for less than one year. It is somewhat surprising that so many are operated after more than one year.
When do surgeons think it is best to operate? Nearly half say around 4–8 weeks. This aligns well with earlier points that pain at six weeks predicts future outcomes. Therefore, it may be reasonable to consider surgery after six weeks if pain remains severe. Note that this is based on data from the United States, where there may be a greater tendency towards surgery than in Norway (?) (25).
How Satisfied Are Patients After Surgery?
In general, patients are satisfied after disc herniation surgery. In the spine registry, it was found that 90.8% of patients were satisfied with the operation at one year (10).
One thing is satisfaction (people can be really satisfied with ineffective treatment)—but what about perceived improvement?
A Norwegian study showed that two thirds of patients reported that they were “completely recovered” or “much better” one year after surgery. These patients had, on average, a reduction in leg pain of 3.5 on the NPRS and 2.5 on the NPRS for back pain (28). This is also supported by larger studies. These show, regardless of whether patients undergo surgery or conservative treatment (!), that 8% experience no improvement, and that 23% of all sciatica patients have ongoing symptoms that fluctuate over time (29).
What Else Influences the Outcome of Surgery?
Weight?
Patients with obesity can expect somewhat poorer results after spinal surgery—but not by much. A high BMI should therefore not delay surgery when there is otherwise a clear indication (10).
Native Language, Ethnicity, and Education?
Good communication about the health problem and what can be achieved with surgery is important. The success rate of lumbar disc surgery is unfortunately 10% lower in patients with a native language other than Norwegian (in Norway). With the use of interpreters, communication can be improved and, hopefully, outcomes as well (10). Lower levels of education are also associated with poorer surgical outcomes (10).
Other factors?
Results from the SPORT study showed poorer outcomes in patients with pain in other joints, smokers and those with depression at the start of treatment (18). Smoking is associated with poorer surgical outcomes. In larger operations, surgeons often require or recommend smoking cessation (10).
Does Location Affect the Outcome?
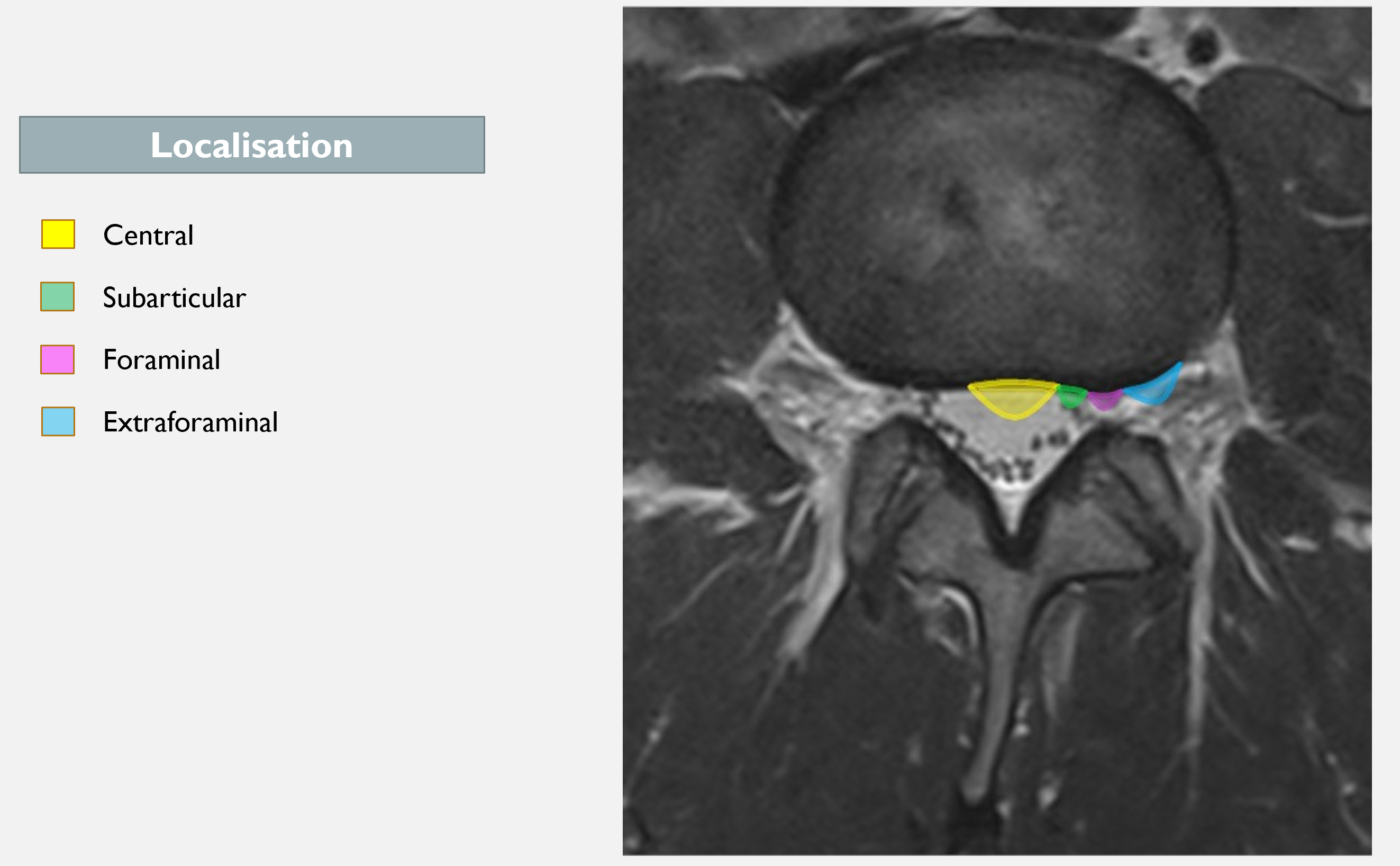
We know that most disc herniations occur in the subarticular region (3 out of 4). According to the SPORT study, prognosis is worse for all types of herniations other than subarticular (18). When they talk about other herniations I do not believe this refers to central herniations, as these less commonly cause symptoms (unless it is a very large herniation causing cauda equina syndrome). Rather, this refers to foraminal and extraforaminal herniations.
Patients with foraminal and extraforaminal herniations may have a more severe symptom profile, as disc material can protrude into a narrower canal with limited space for nerve displacement. The dorsal root ganglion is also located here, which is a potentially pain-sensitive structure (30,31). Other studies also show that these patients have somewhat poorer outcomes from both surgery and conservative treatment (32,33).
But I think it all depends on a lot of factors if they are going to be painful or not.
Size and Type of Herniation?
We know that location can influence outcome—but what about the type of herniation? Does this affect how well patients do after surgery?
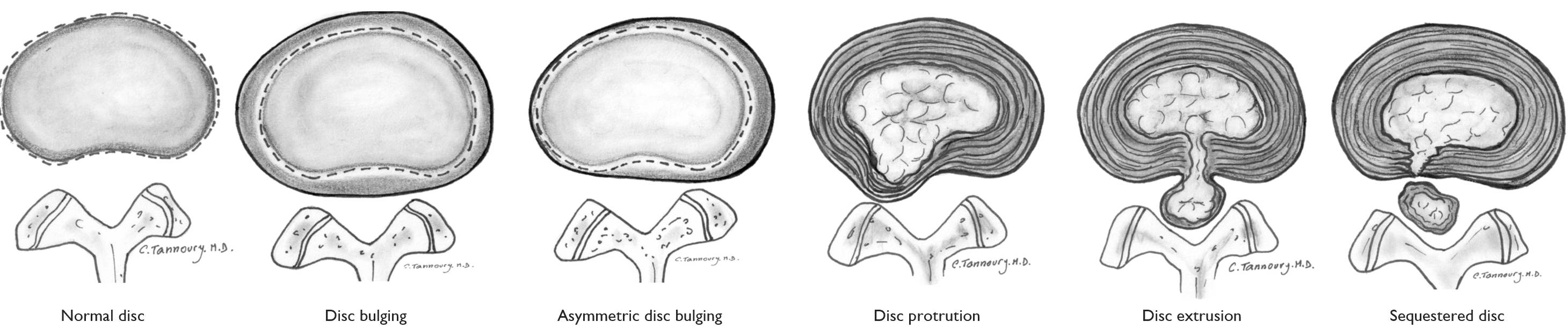
Protrusion is a common finding on MRI, both in those with and without pain (35,36). In my view, it is less common for a protrusion to cause radicular pain and radiculopathy, except in cases where a larger protrusion occurs in the intervertebral foramen or where there are significant degenerative changes in the spine (annulus, facet joints, disc). Therefore, these are rarely operated on.
This is also reflected in studies comparing surgery across different types of herniations. Patients with a contained herniation (where the “car tyre” has not ruptured), likely corresponding to a protrusion, have poorer outcomes after surgery.
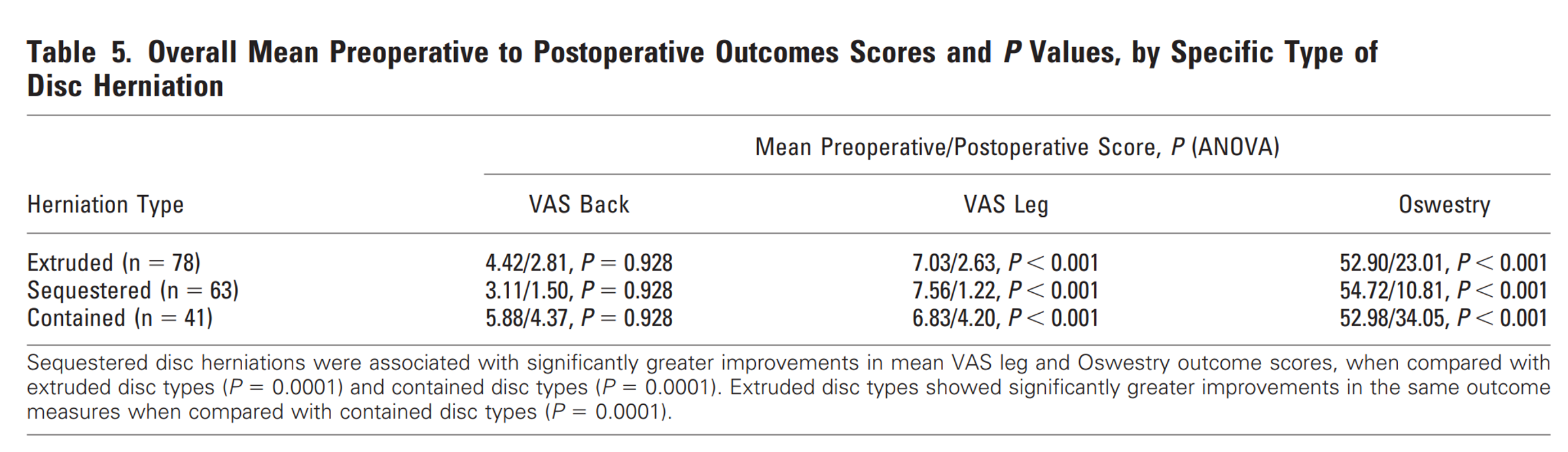
What did they find? Patients with sequestration had very high pain levels initially, but after surgery, the average NPRS was only 1.2. Those with extrusion also had significant pain before surgery, which decreased to an NPRS of 2.6 after surgery. Patients with protrusion had the poorest outcomes, with leg pain at NPRS 4.2 postoperatively. They also had more back pain and worse Oswestry scores (37). If you have a protrusion, one should perhaps more strongly consider avoiding surgery, or at least adjust expectations.
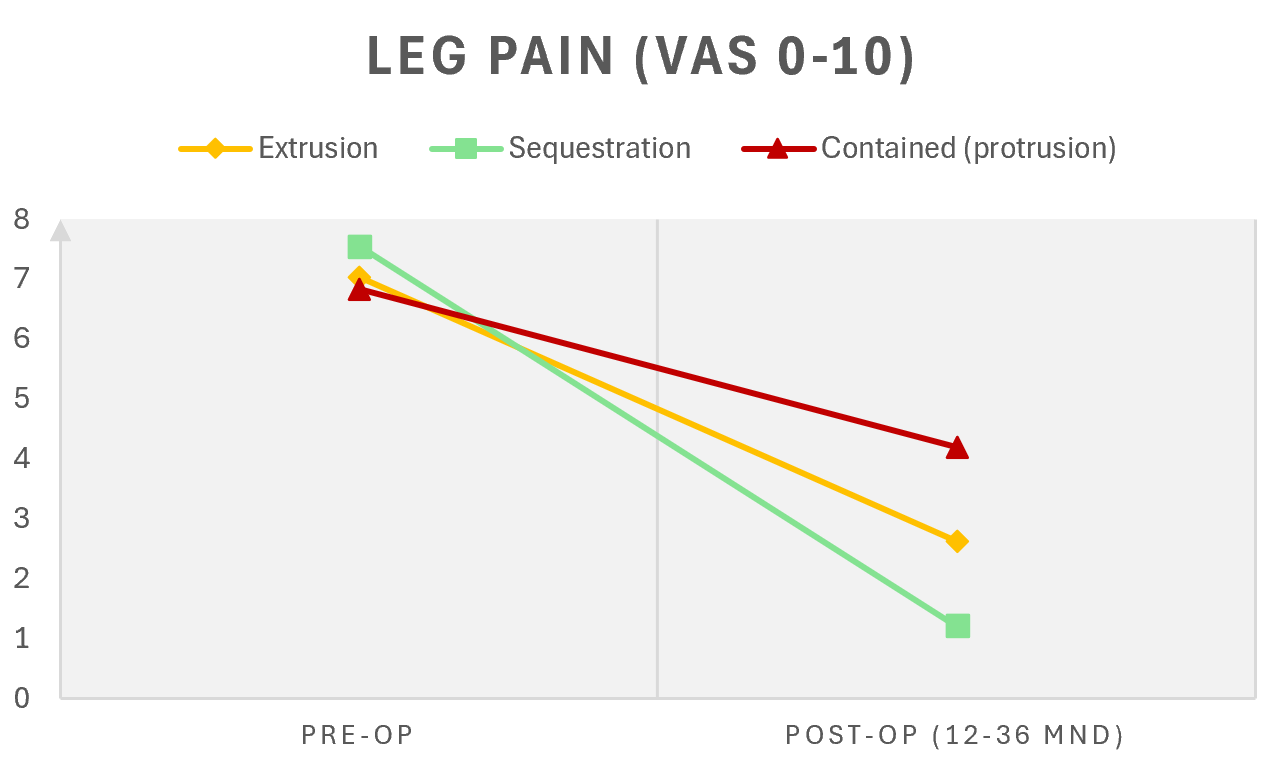
Extrusion is rarely asymptomatic and often causes radicular pain (36,38). Sequestration often involves disc material that has passed through the posterior longitudinal ligament and entered the spinal canal (39). In the study mentioned above by Dewing et al., patients with extrusion and sequestration had significantly better outcomes compared to those operated on for protrusion (37). The question is whether the latter group should have been operated on at all, given that they also have a good prognosis with conservative treatment.
If we look again at sequestration: in a study comparing surgery and conservative treatment for this type of herniation, spontaneous regression was observed after six months in the conservatively treated group. Initially, those who underwent surgery had less pain and functional limitation, but after six months there was no difference. Paradoxically, larger herniations (sequestrations) therefore have a better prognosis (40).
Another study (41) supports the idea that one should be cautious about operating on small disc herniations. By small herniations, this refers to contained herniations (where the disc wall has not ruptured), often protrusions. In this study, patients were divided into four groups based on the size of the herniation (see table and figure below).
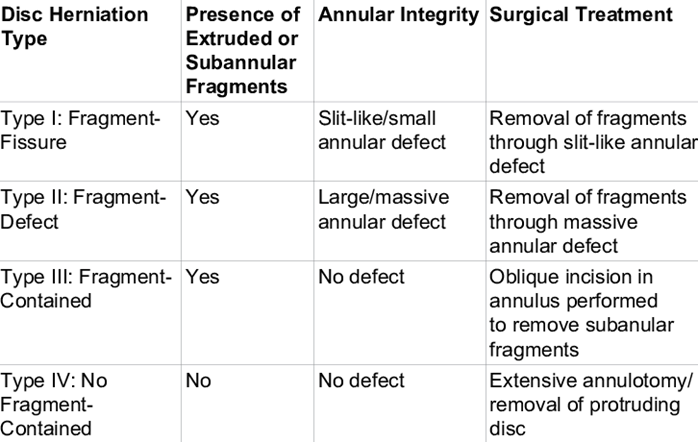
This study showed extremely poor outcomes following surgery for herniations smaller than 5 mm (antero-posterior diameter), and suggested that a herniation larger than 8 mm is needed for relatively good results. This is illustrated in the graph below. In the group with small, contained herniations, 37.5% experienced recurrence of sciatica (41).
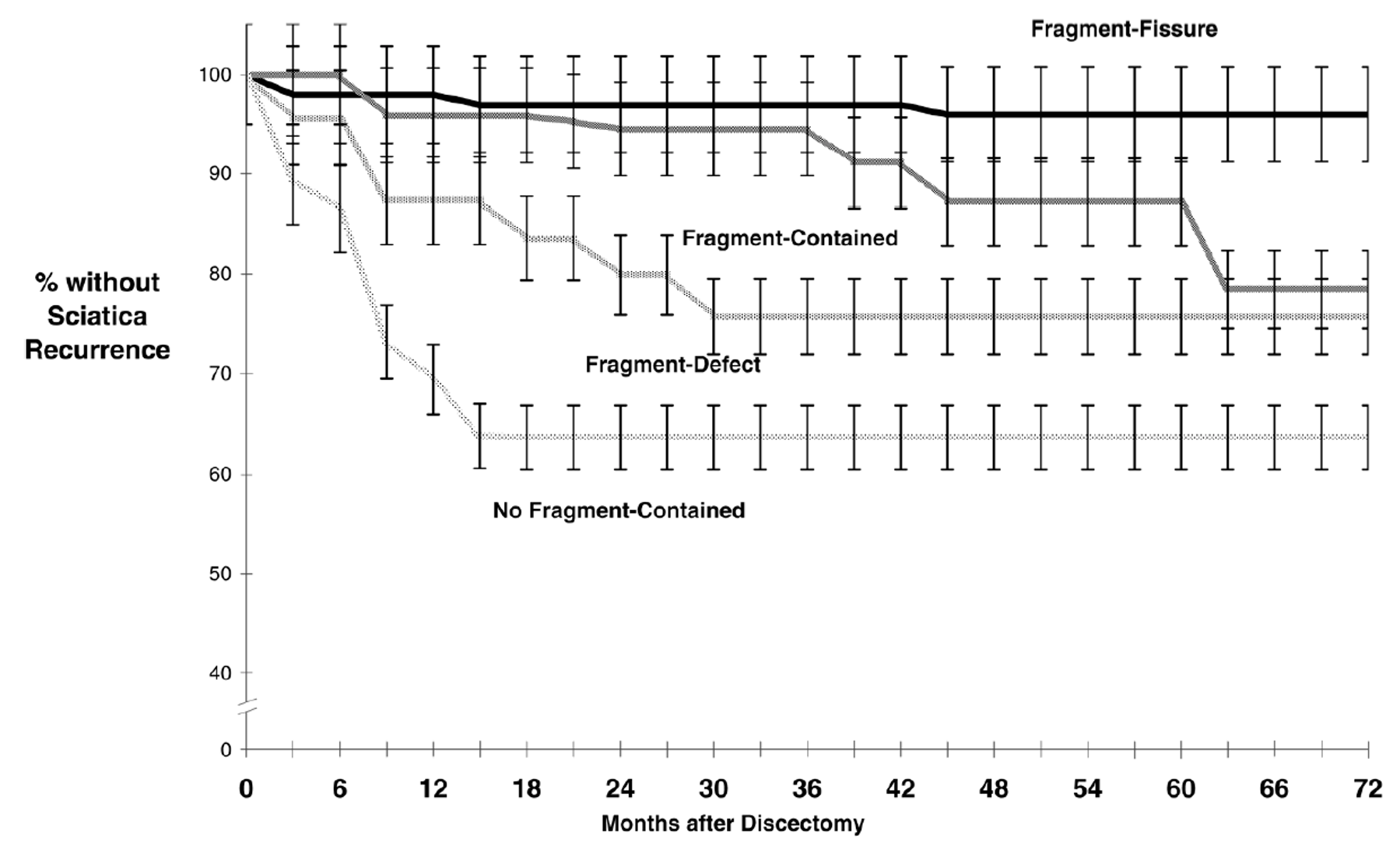
The study also challenges the idea that larger herniations are always better for prognosis. Yes, it is generally favourable when the disc wall has ruptured and disc material has extruded, but the very largest type (fragment-defect) may not be as favourable either. In cases with a complete defect of the disc wall, there is an increased risk of future sciatica (27.3%), as well as a higher risk of recurrent herniation (around 1 in 5 require reoperation) (41). A small note here is that this is an older study, from 2003, and there have likely been significant advancements in surgical techniques since then.
On the other hand, there are also studies suggesting that size may not be as important. A study from 2019 examined whether the size of the herniation predicted the type of treatment required—surgery or conservative management (patients with significant motor deficits and cauda equina were excluded). They found no association between the size of the herniation and whether surgery was needed (42).
So, this is not black and white. I believe it depends on the location of the herniation and how much space the nerve has available—as well as other factors such as general health, comorbidities, and psychosocial factors. You can have a very large herniation extending into the spinal canal without compressing any nerve tissue, and you can have a small herniation in the intervertebral foramen causing significant nerve compression. One should be cautious about operating on small herniations—the consequences of surgery may outweigh the benefits. Herniations where the disc wall has ruptured tend to have a better prognosis.
Persistent Weakness After Surgery?
Patients with motor deficits due to disc herniation are often concerned about whether muscle strength will return—for example, in the calf muscles following an S1 nerve root compression. In clinical practice, I see that many patients do regain muscle strength, but unfortunately some do not—and are left with permanent paresis or paralysis.
As with most things, many factors play a role, and one of the most important is time to surgery. As mentioned, some hospitals recommend specialist assessment within 72 hours of onset of motor deficit, while others recommend surgery within one week (while some may say longer?). Personally, I prefer to have patients with newly developed motor weakness assessed in hospital as quickly as possible, and then the surgeon and the patient can make the decision what to do.
If a patient presents with a foot drop that has been present for one year, it is unlikely that surgery will resolve it (although one can never be completely certain), and hospitals will often consider it too late. However, a referral can always be sent, and the final decision can be made by the specialist team.

What does the research say about the likelihood of regaining strength after surgery? With a grade 4 motor deficit, 84% regain full strength, whereas with grade 3 or lower, the likelihood is around 55% (43). This is why early assessment is important. Some patients should undergo early surgery to avoid permanent nerve damage.
Herniation Content
The content of the herniation may be important in determining whether surgery is needed or not. Some herniations can be softer, more gelatinous, and will resorb relatively quickly—leading to faster recovery—while others may have a firmer, more rubber-like consistency, almost becoming calcified. It is conceivable that the body has more difficulty resorbing these harder herniations. I heard this discussed in the podcast Vondt, in an episode on spine surgery—very interesting.
It is therefore incorrect to think that all herniation material consists of “soft” nucleus pulposus that comes out of the annulus fibrosus. It can also contain cartilage, endplate, and bone, and if the herniation is very large, it may become covered by granulation tissue (39,44,45).

What About the Level?
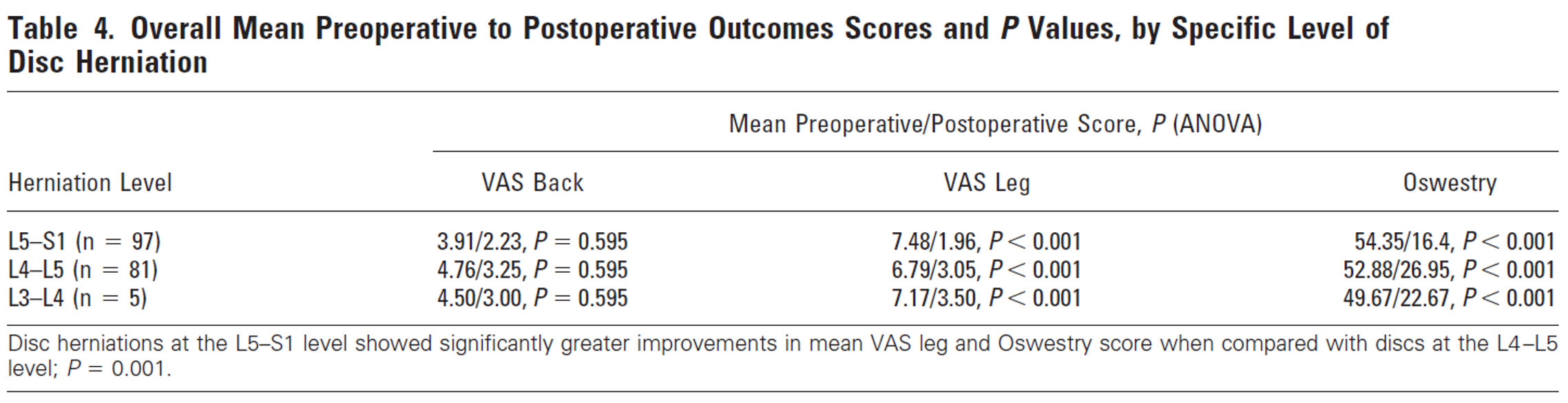
Is there a difference in prognosis depending on the level of the herniation? In a study by Dewing et al. (37), it was found that patients with an L5–S1 herniation had significantly less leg pain and a lower Oswestry score after surgery compared to those with L4–L5 herniations. The authors suggest that there may be a lower risk of recurrent herniation at the lowest spinal level due to stabilising ligaments between the pelvis and lumbar spine. It is also noted that the intervertebral foramen for the S1 nerve root is larger, making it less affected by disc degeneration and foraminal narrowing (37).
What Is the Risk of Recurrent Herniation After Surgery?
In the literature, it is reported that between 2–18% experience a recurrent herniation after surgery. In one study, patients with a wider annular defect (greater than 6 mm) had a 27% risk of recurrence, compared to 4.8% in the remaining group (although this group was relatively small) (46). In Norway, approximately 5% are re-operated within one year (16).
Surgeons face a dilemma during surgery. If a large amount of disc material is removed, there is a higher risk of disc degeneration and pain in the first year. If less disc material is removed, the disc may remain more “healthy,” but the risk of recurrent herniation is higher (9% vs 18%) (46). Despite the higher risk of recurrence in the group where less material is removed, these patients report higher satisfaction two years after surgery (47).
What About Second or Multiple Surgeries?
In another systematic review, around 6% of patients underwent reoperation for herniation at the same level (48). This aligns well with Norwegian data, which show that approximately 5% are re-operated within one year (2.1% of these within 90 days) (16). According to the spine registry, 1.9% had undergone more than two surgeries for disc herniation in 2023 (10).
Multiple surgeries for spinal problems have been shown to have minimal effect (10). Several studies have found an association between repeated spinal surgeries and poorer outcomes (49). A Norwegian study examining disc herniation and lumbar spinal stenosis showed quite clearly that the likelihood of achieving an acceptable outcome after 12 months (PASS = >22 ODI score) decreases substantially with each additional surgery (49).
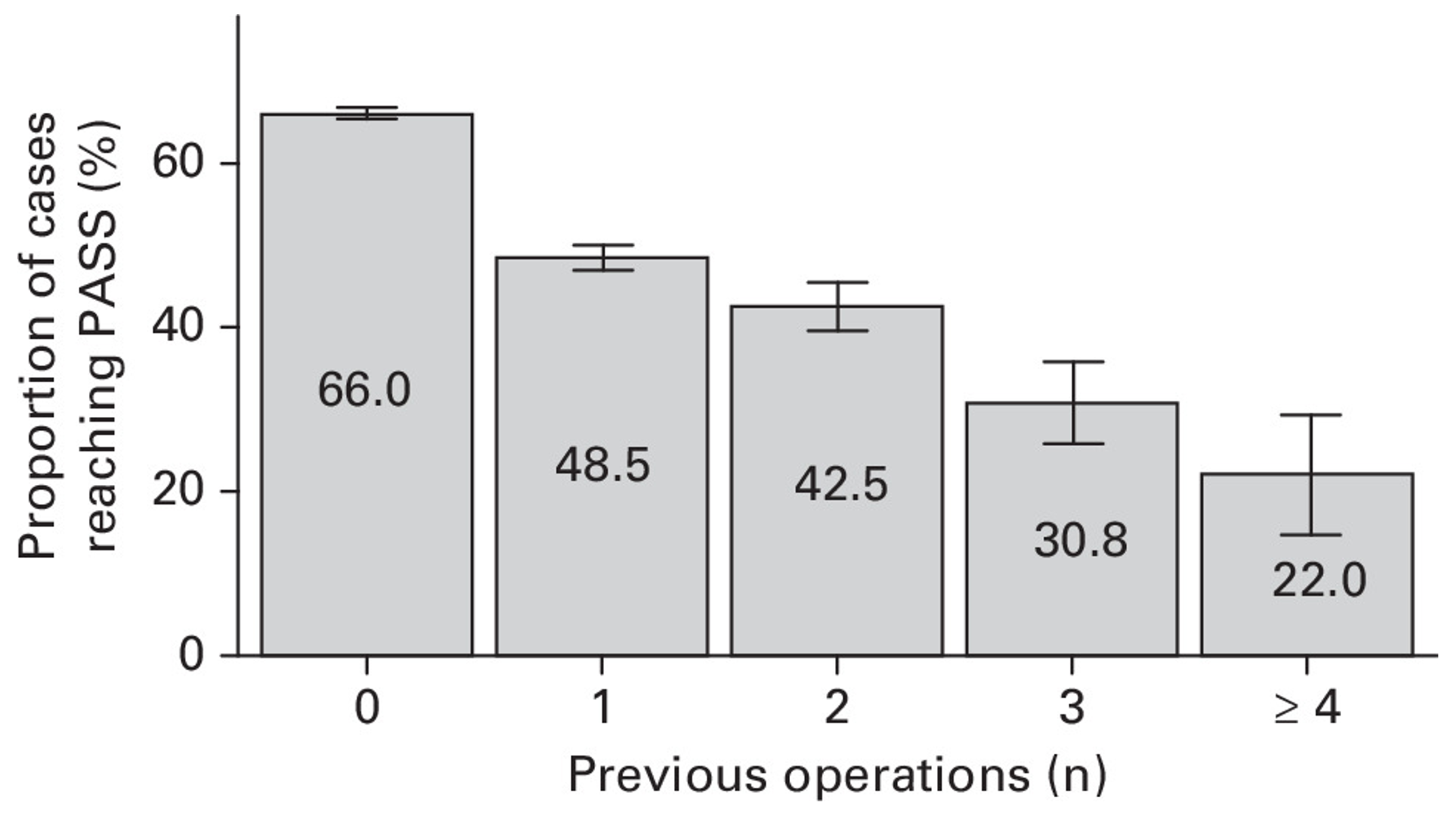
One should therefore be cautious about repeated spinal surgeries—the more times you are operated on, the lower your expectations should be.
Asymptomatic Recurrent Herniation Is Common
It is also important to remember that asymptomatic recurrent herniation is common—that is, a herniation that does not cause symptoms. If you have undergone surgery, develop new pain, have a follow-up MRI, and a recurrent herniation is seen—it is not necessarily the cause of your symptoms, nor does it automatically mean that another operation is needed.
In one study, 1.5% had a recurrent herniation after one year, and 5.1% after two years (46). In another study, 23% had a recurrent herniation two years after surgery, but more than half of these were asymptomatic—without symptoms. Having an asymptomatic herniation had no consequences at two years (50).
Therefore—as always—MRI findings must be interpreted in conjunction with the clinical examination.
Having a recurrent herniation after surgery is not uncommon, and it does not mean that you need another operation. Asymptomatic herniations can be ignored (50).
Complications?
Another factor that must be included in the equation is the risk of adverse events and complications associated with surgery. In a study by Bailey, 9 out of 128 patients experienced complications, and one patient required reoperation (22).
In a large Norwegian study (including as many as 34,639 operations), 6.7% experienced an adverse event related to disc surgery. This was more frequent in older patients and those with more comorbidities (16). In this study, 2.7% had a surgical complication, 2.1% required reoperation, while 2.4% had a non-surgical hospital admission (16). Infection (1.6%), dural tear (1%), and haematoma (0.6%) are among the most common complications (51).
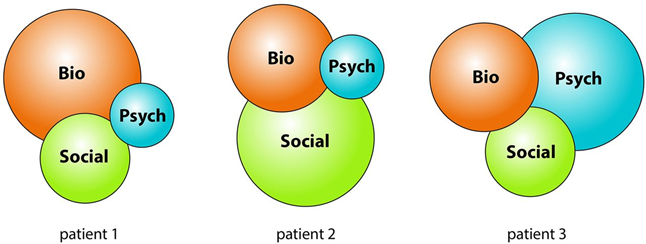
Psychosocial Factors
As physiotherapists, we are always taught to consider the “whole patient” and to make a biopsychosocial assessment. We learn that psychosocial factors influence prognosis and pain. But what about radicular pain? Schmid et al., in their 2020 article, actually state that it is debated or uncertain whether psychosocial factors influence prognosis in conservative treatment (34).
But what about surgery?
Several studies have shown that patients with depression and anxiety have an increased risk of poorer outcomes after spinal surgery. Increased risk has been demonstrated for reduced quality of life, longer hospital stays, greater use of healthcare services, poorer walking ability, higher risk of delirium, increased pain, and increased mortality (52). This means that when considering surgery, one should have a thorough conversation with the patient and also explore psychosocial factors.
Anxiety and depression are the most common mental health conditions associated with back and neck pain. A large multinational study (85,088 patients) found nearly double the risk of anxiety and mood disorders in individuals with chronic back and neck pain, regardless of country. Another study (118,533 individuals) showed that 19.8% of those with chronic low back pain had severe depression, compared to 5.9% in the pain-free population (53).
The question is often: are patients depressed because of the pain, or did they develop pain as a result of depression and its consequences?
Some researchers have attempted to answer this. A prospective study of 9,909 adults without prior low back pain found that those with depression had nearly a threefold increased risk of developing chronic low back pain over two years. There are likely multiple mechanisms behind this relationship. Those with depression in this group were less likely to be employed, rated their health as poorer, and had more health problems overall (54).
Another perspective comes from a Dutch study (5,303 individuals), which found that people with moderate to severe pain had twice the risk of developing anxiety or mood disorders. Interestingly, spontaneous improvement in mental health conditions has been observed after successful surgical interventions, suggesting a bidirectional relationship between pain and mental health (53).
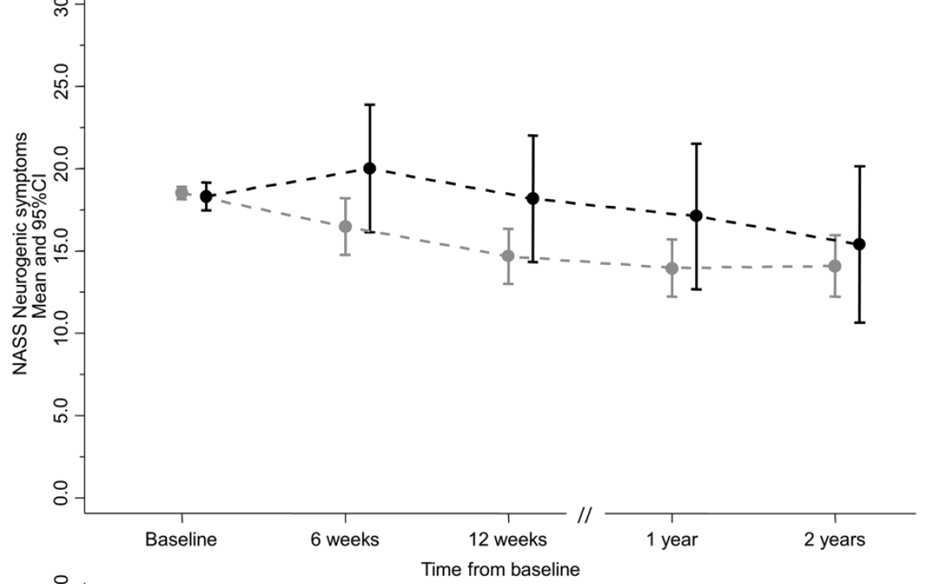
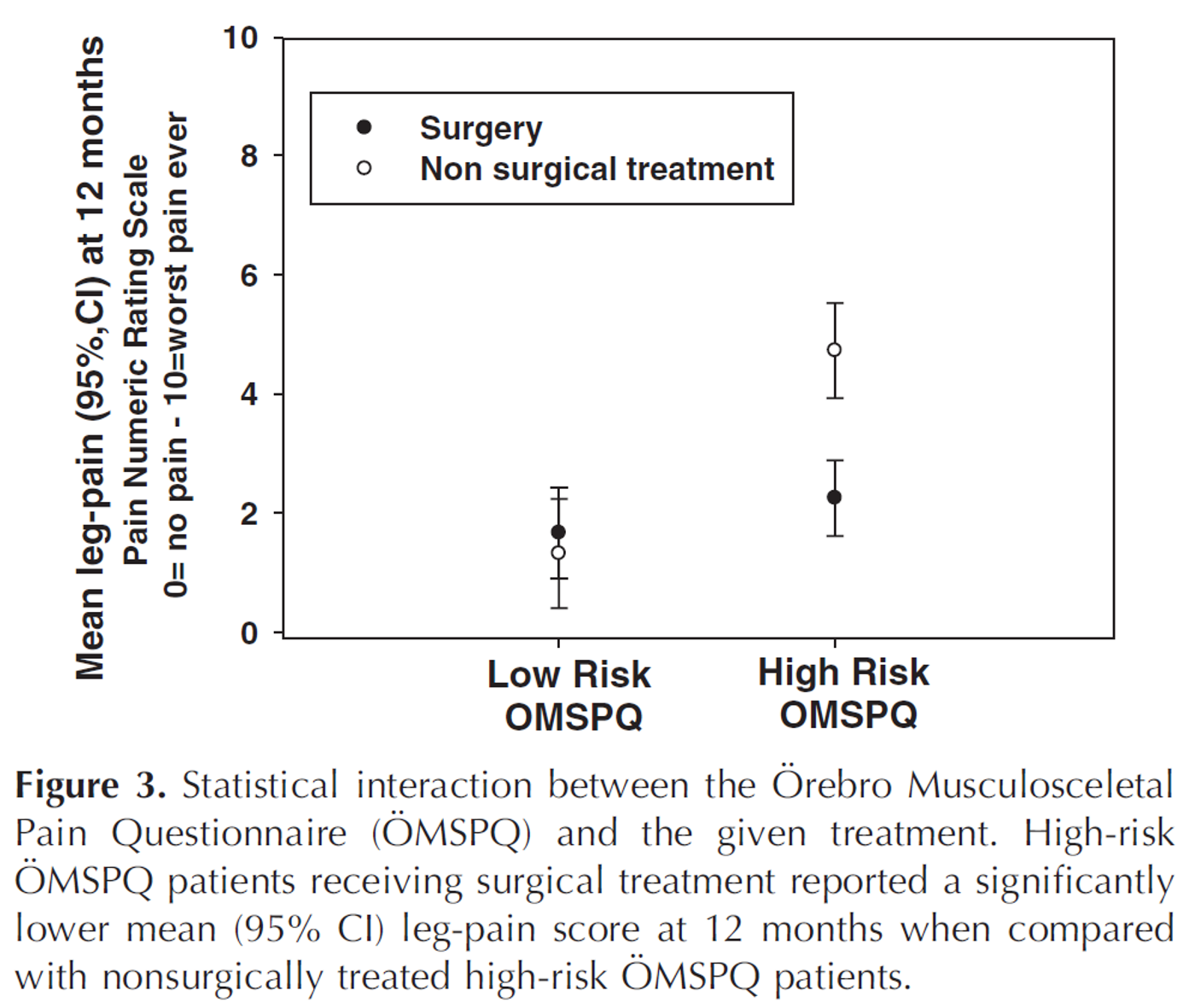
This is also seen in studies of patients admitted to hospital due to very painful sciatica. Those who score high on the Örebro questionnaire have a higher likelihood of leg pain than those with lower scores, both with and without surgery—but the difference is particularly clear in those who are not operated on. Patients with a high-risk Örebro score therefore experience significantly more leg pain without surgery (see below) (23). This highlights that people with higher levels of psychosocial risk factors should also be considered when evaluating for surgery. Patients should not be unnecessarily stigmatised.
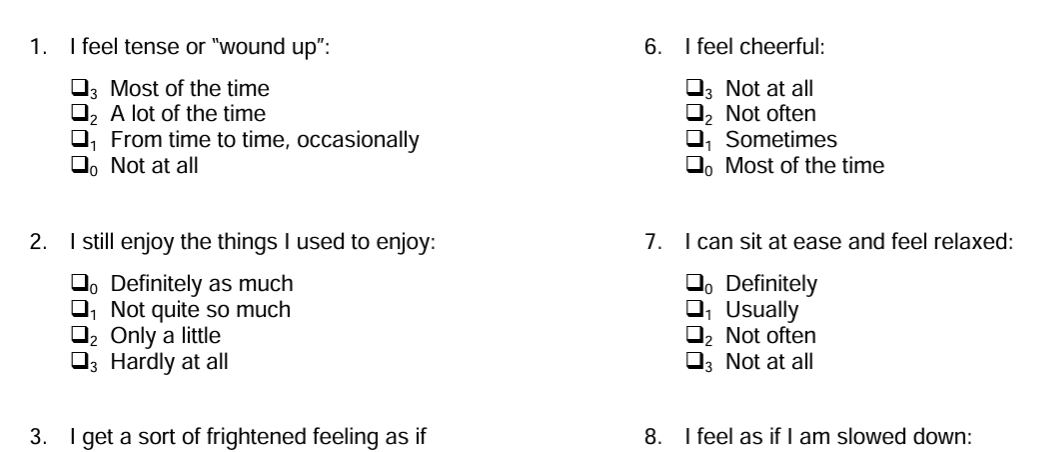
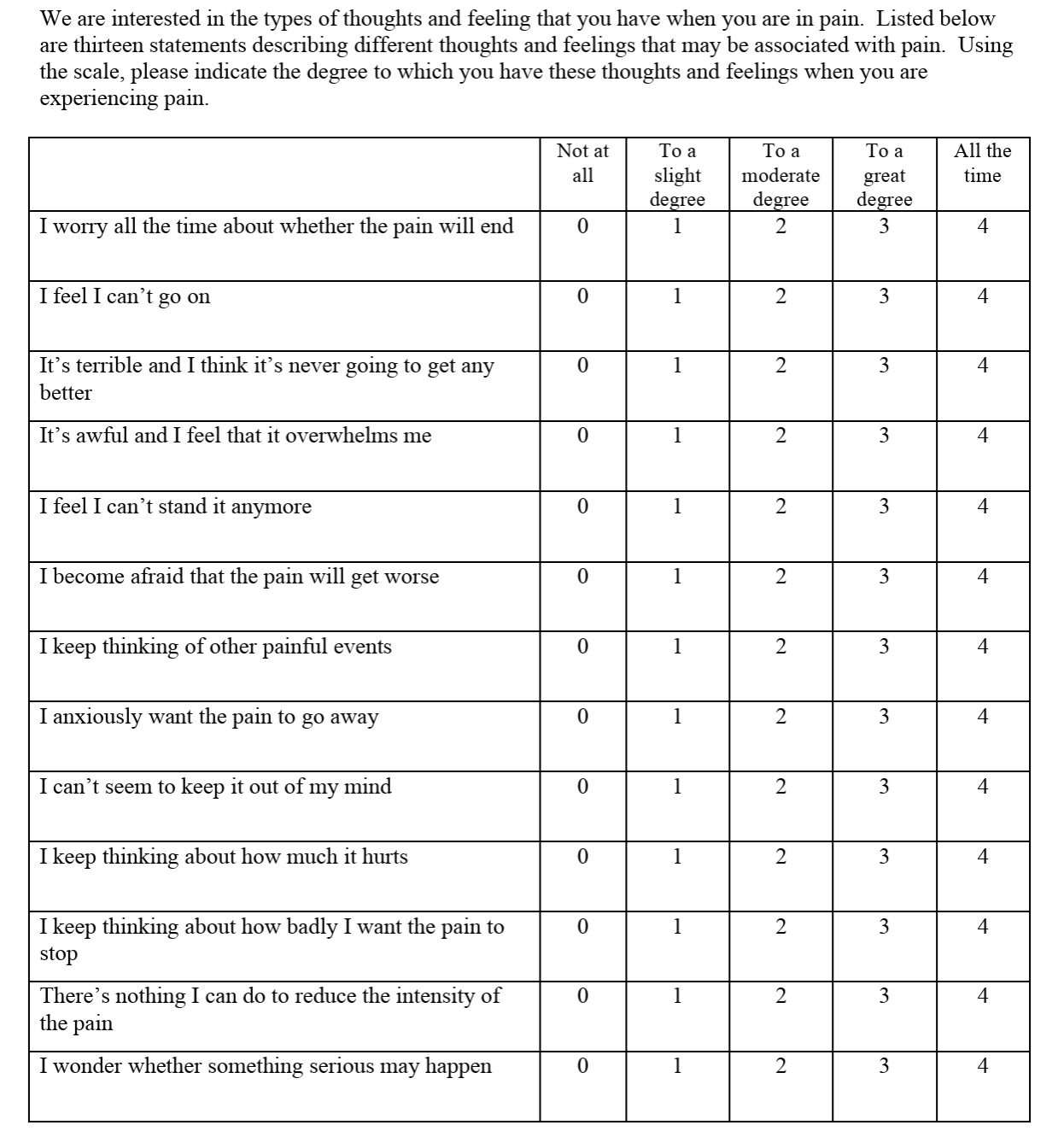
Use the Hospital Anxiety and Depression Scale (HADS) or the Örebro questionnaire to assess this in the patient (55).
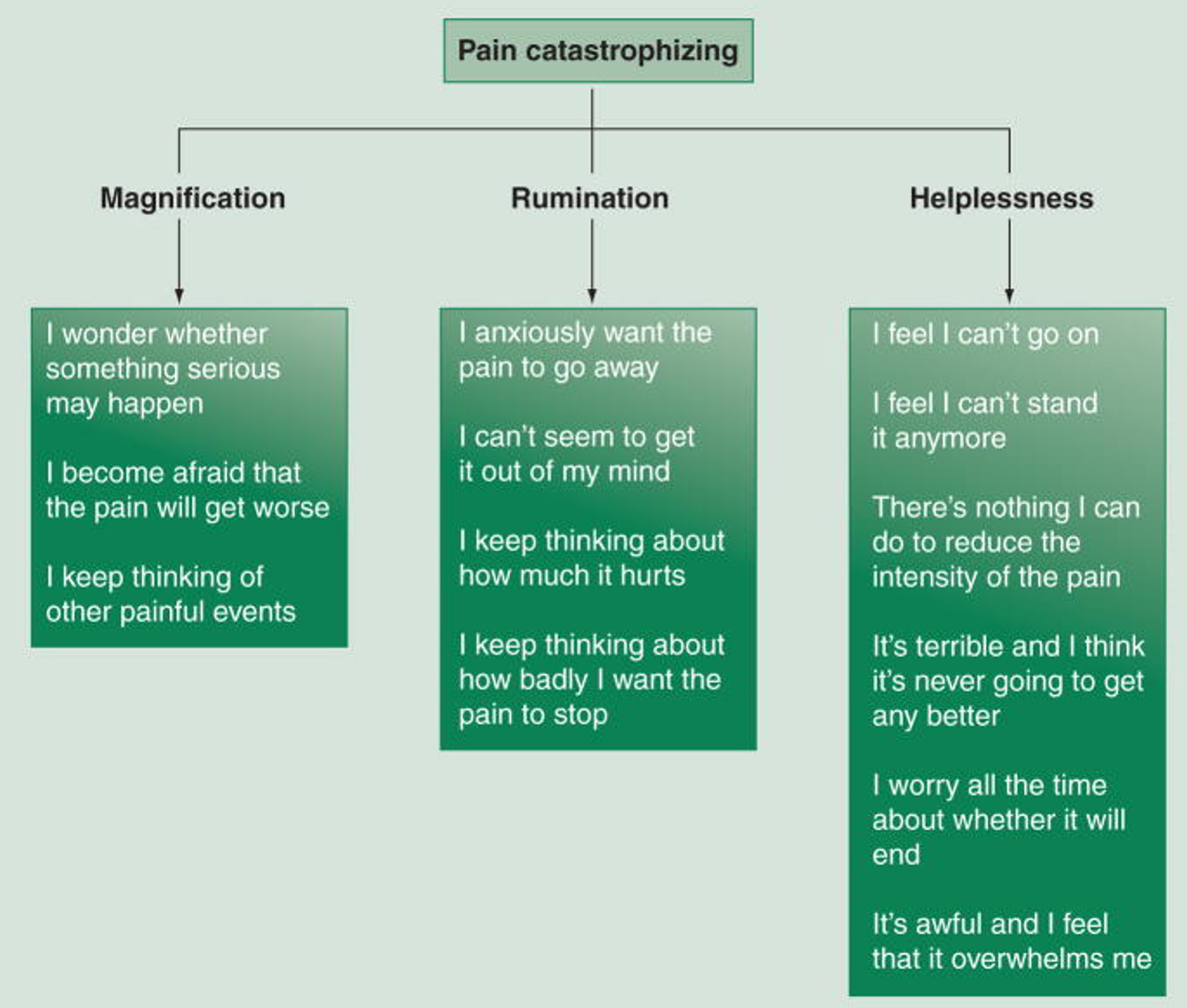
Pain Catastrophising
One of the most important psychosocial factors to assess is pain catastrophising, which is perhaps the strongest predictor of pain and function after surgery (and in musculoskeletal conditions in general) (56–58). Pain catastrophising is characterised by an exaggerated perception of the threat of pain (magnification), feelings of helplessness in relation to pain, and an inability to stop thinking about the pain (rumination) (56,57). Pain catastrophising is associated with emotional distress, poorer treatment response, and negative clinical outcomes such as prolonged disability and opioid overuse (56).
Research consistently shows that higher levels of pain catastrophising are associated with increased pain intensity across different populations and conditions (56). Pain catastrophising has been identified as a key factor in the development of persistent back pain after spinal surgery (60,61). A high score on the Pain Catastrophizing Scale (PCS) has been shown to predict a chronic pain condition, defined as persistent disability after lumbar surgery (61). Studies also indicate a bidirectional relationship between pain catastrophising and pain, where changes in catastrophising influence pain outcomes and vice versa (56).
There is, however, some controversy surrounding the concept of pain catastrophising. In an article by Petrini and Arendt-Nielsen from 2020, they state that there is no clear consensus on the definition of pain catastrophising or what it represents as a concept (63).
Regardless, I believe that as a clinician, you should explore the degree of pain catastrophising. If there is a high PCS score, it may be reasonable to delay surgery (?) (of course, surgery should still be performed in cases of significant motor deficit due to disc herniation). If the clinician has competence in this area (e.g. cognitive therapy), one can explore and address the patient’s fears; otherwise, referral to a general practitioner and/or psychologist may be appropriate.
However, when looking at interventions aimed at reducing PCS, studies actually show similar effects from physical activity and psychological treatment. The mechanisms are therefore uncertain and non-specific (56,63).
A recent systematic review by Lanini et al. suggests that psychological intervention prior to surgery may be beneficial. They write (16):
“Our findings confirm that psychological interventions can help improve surgical outcomes by positively influencing patients’ metabolic surgical stress response. A multidisciplinary approach integrating physical and non-physical therapies can be considered a good strategy to improve surgical outcomes in the perioperative period.”
Final Remarks on Psychosocial Factors
It is important for us as clinicians to explore psychosocial factors—but remember: “you can still break your leg even if you have depression.” In other words, sometimes—and often—the radicular pain itself is the main problem.
Summary
- Very few patients should undergo surgery for disc herniation, and if you have more back pain than leg pain, you should definitely not be operated on.
- Only those with newly developed, significant or progressive motor deficit in the leg, or cauda equina syndrome, should be admitted to hospital as an emergency.
- The “grey zone” patients (no pronounced motor deficit ≥4 and persistent, painful sciatica, >3 NPRS) can be managed with a wait-and-see approach.
- The level of pain after 6 weeks is predictive of pain at one year. These patients should therefore definitely be followed up at 6–8 weeks, with increased clinical focus—and, if necessary, referral for surgical assessment.
- On average, surgery appears to be as effective as conservative treatment after one year, but there are many “cross-overs” in these studies. Each case should be assessed individually—every patient is unique.
- It is likely less advisable to operate on small herniations, but this depends on how much space the nerve has to move.
- If surgery is considered, it should ideally be performed within 6–12 months.
- Remember that surgery always carries some risk, even if low. Avoid multiple back surgeries if possible.
- If surgery is being considered, assess pain catastrophising and Örebro scores. These factors may influence prognosis—but remember: “even depressed patients can break their leg.”
References
1. Oliveira CB, Maher CG, Pinto RZ, Traeger AC, Lin CWC, Chenot JF, mfl. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. 1. november 2018;27(11):2791–803.
2. Koes BW, van Tulder MW, Peul WC. Diagnosis and treatment of sciatica. BMJ. 23. juni 2007;334(7607):1313–7.
3. Hartvigsen L, Hestbaek L, Lebouef-Yde C, Vach W, Kongsted A. Leg pain location and neurological signs relate to outcomes in primary care patients with low back pain. BMC Musculoskelet Disord. 31. mars 2017;18(1):133.
4. Konstantinou K, Dunn KM. Sciatica: review of epidemiological studies and prevalence estimates. Spine. 15. oktober 2008;33(22):2464–72.
5. M H, O I, K S, T M, P K, J K, mfl. Lumbar disc syndrome in Finland. J Epidemiol Community Health [Internett]. september 1987 [sitert 16. oktober 2024];41(3). Tilgjengelig på: https://pubmed.ncbi.nlm.nih.gov/2965207/
6. van der Windt DA, Simons E, Riphagen II, Ammendolia C, Verhagen AP, Laslett M, mfl. Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain. Cochrane Database Syst Rev. 17. februar 2010;(2):CD007431.
7. Weber H. Lumbar disc herniation. A controlled, prospective study with ten years of observation. Spine. mars 1983;8(2):131–40.
8. Weber H. Hva du bør vite om ryggplager. Oslo: Grøndahl; 1989.
9. Fjeld OR. Symptomatic lumbar disc herniation treated in hospitals – Prognosis of unfavourable surgical events and persistent leg-pain [PHD]. [Institute of Clinical Medicine, Faculty of Medicine, University of Oslo]: University of Oslo; 2020.
10. Solberg TK, Ingebrigtsen T, Olsen LR, Thyrhaug AM. Årsrapport 2023 Nasjonalt kvalitetsregister for ryggkirurgi: Resultater og forbedringstiltak. Septentrio Rep [Internett]. 4. november 2024 [sitert 6. januar 2025];(1). Tilgjengelig på: https://septentrio.uit.no/index.php/SapReps/article/view/7850
11. Hermansen E, Myklebust TÅ, Austevoll IM, Rekeland F, Solberg T, Storheim K, mfl. Clinical outcome after surgery for lumbar spinal stenosis in patients with insignificant lower extremity pain. A prospective cohort study from the Norwegian registry for spine surgery. BMC Musculoskelet Disord. 22. januar 2019;20(1):36.
12. Katz JN, Zimmerman ZE, Mass H, Makhni MC. Diagnosis and Management of Lumbar Spinal Stenosis: A Review. JAMA. 3. mai 2022;327(17):1688–99.
13. Jacobs WCH, van Tulder M, Arts M, Rubinstein SM, van Middelkoop M, Ostelo R, mfl. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systematic review. Eur Spine J. 1. april 2011;20(4):513–22.
14. Gugliotta M, Costa BR da, Dabis E, Theiler R, Jüni P, Reichenbach S, mfl. Surgical versus conservative treatment for lumbar disc herniation: a prospective cohort study. BMJ Open. 1. desember 2016;6(12):e012938.
15. Peul WC, van den Hout WB, Brand R, Thomeer RTWM, Koes BW. Prolonged conservative care versus early surgery in patients with sciatica caused by lumbar disc herniation: two year results of a randomised controlled trial. BMJ. 14. juni 2008;336(7657):1355–8.
16. Fjeld OR, Grøvle L, Helgeland J, Småstuen MC, Solberg TK, Zwart JA, mfl. Complications, reoperations, readmissions, and length of hospital stay in 34 639 surgical cases of lumbar disc herniation. Bone Jt J. april 2019;101-B(4):470–7.
17. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-Term Outcomes of Surgical and Nonsurgical Management of Sciatica Secondary to a Lumbar Disc Herniation: 10 Year Results from the Maine Lumbar Spine Study: Spine. april 2005;30(8):927–35.
18. Kerr D, Zhao W, Lurie JD. What Are Long-term Predictors of Outcomes for Lumbar Disc Herniation? A Randomized and Observational Study. Clin Orthop. juni 2015;473(6):1920–30.
19. Wang Y, Dai G, Jiang L, Liao S. The incidence of regression after the non-surgical treatment of symptomatic lumbar disc herniation: a systematic review and meta-analysis. BMC Musculoskelet Disord. 10. august 2020;21(1):530.
20. Gifford L. Aches and pains. 2014.
21. Schoenfeld AJ, Kang JD. Decision Making for Treatment of Persistent Sciatica. N Engl J Med. 19. mars 2020;382(12):1161–2.
22. Bailey CS, Rasoulinejad P, Taylor D, Sequeira K, Miller T, Watson J, mfl. Surgery versus Conservative Care for Persistent Sciatica Lasting 4 to 12 Months. N Engl J Med. 19. mars 2020;382(12):1093–102.
23. Fjeld O, Grotle M, Siewers V, Pedersen LM, Nilsen KB, Zwart JA. Prognostic Factors for Persistent Leg-Pain in Patients Hospitalized With Acute Sciatica. Spine. mars 2017;42(5):E272–9.
24. Fernandez M, Ferreira ML, Refshauge KM, Hartvigsen J, Silva IRC, Maher CG, mfl. Surgery or physical activity in the management of sciatica: a systematic review and meta-analysis. Eur Spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc. 2016;25(11):3495–512.
25. Siccoli A, Staartjes VE, de Wispelaere MP, Schröder ML. Association of time to surgery with leg pain after lumbar discectomy: is delayed surgery detrimental? J Neurosurg Spine. 25. oktober 2019;32(2):160–7.
26. Rihn JA, Hilibrand AS, Radcliff K, Kurd M, Lurie J, Blood E, mfl. Duration of symptoms resulting from lumbar disc herniation: effect on treatment outcomes: analysis of the Spine Patient Outcomes Research Trial (SPORT). J Bone Joint Surg Am. 19. oktober 2011;93(20):1906–14.
27. Lærum E, Brox JI, Storheim K. Nasjonale kliniske retningslinjer. Korsryggsmerter – med og uten nerverotaffeksjon. FORMI Formidlingsenheten Muskel- Og SkjelettlidelserSosial- Og Helsedirektoratet. 2007;
28. Solberg T, Johnsen LG, Nygaard ØP, Grotle M. Can we define success criteria for lumbar disc surgery?: Estimates for a substantial amount of improvement in core outcome measures. Acta Orthop. januar 2013;84(2):196–201.
29. Lequin MB, Verbaan D, Jacobs WCH, Brand R, Bouma GJ, Vandertop WP, mfl. Surgery versus prolonged conservative treatment for sciatica: 5-year results of a randomised controlled trial. BMJ Open. 28. mai 2013;3(5):e002534.
30. Epstein NE. Foraminal and far lateral lumbar disc herniations: surgical alternatives and outcome measures. Spinal Cord. oktober 2002;40(10):491–500.
31. Park HW, Park KS, Park MS, Kim SM, Chung SY, Lee DS. The Comparisons of Surgical Outcomes and Clinical Characteristics between the Far Lateral Lumbar Disc Herniations and the Paramedian Lumbar Disc Herniations. Korean J Spine. september 2013;10(3):155–9.
32. Lee JH, Lee SH. Clinical and Radiological Characteristics of Lumbosacral Lateral Disc Herniation in Comparison With Those of Medial Disc Herniation. Medicine (Baltimore) [Internett]. 18. februar 2016 [sitert 23. mars 2020];95(7). Tilgjengelig på: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4998615/
33. Khan JM, McKinney D, Basques BA, Louie PK, Carroll D, Paul J, mfl. Clinical Presentation and Outcomes of Patients With a Lumbar Far Lateral Herniated Nucleus Pulposus as Compared to Those With a Central or Paracentral Herniation. Glob Spine J. august 2019;9(5):480–6.
34. Schmid AB, Fundaun J, Tampin B. Entrapment neuropathies: a contemporary approach to pathophysiology, clinical assessment, and management. Pain Rep [Internett]. 22. juli 2020 [sitert 24. september 2020];5(4). Tilgjengelig på: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7382548/
35. Brinjikji W, Luetmer PH, Comstock B, Bresnahan BW, Chen LE, Deyo RA, mfl. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. Am J Neuroradiol. april 2015;36(4):811–6.
36. Brinjikji W, Diehn FE, Jarvik JG, Carr CM, Kallmes DF, Murad MH, mfl. MRI Findings of Disc Degeneration are More Prevalent in Adults with Low Back Pain than in Asymptomatic Controls: A Systematic Review and Meta-Analysis. Am J Neuroradiol. desember 2015;36(12):2394–9.
37. Dewing CB, Provencher MT, Riffenburgh RH, Kerr S, Manos RE. The outcomes of lumbar microdiscectomy in a young, active population: correlation by herniation type and level. Spine. 1. januar 2008;33(1):33–8.
38. Suri P, Boyko EJ, Goldberg J, Forsberg CW, Jarvik JG. Longitudinal associations between incident lumbar spine MRI findings and chronic low back pain or radicular symptoms: retrospective analysis of data from the longitudinal assessment of imaging and disability of the back (LAIDBACK). BMC Musculoskelet Disord. 13. mai 2014;15(1):152.
39. Fardon DF, Williams AL, Dohring EJ, Murtagh FR, Gabriel Rothman SL, Sze GK. Lumbar disc nomenclature: version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Spine J Off J North Am Spine Soc. 1. november 2014;14(11):2525–45.
40. Sucuoğlu H, Barut AY. Clinical and Radiological Follow-Up Results of Patients with Sequestered Lumbar Disc Herniation: A Prospective Cohort Study. Med Princ Pract. 18. februar 2021;30(3):244–52.
41. Carragee EJ, Han MY, Suen PW, Kim D. Clinical outcomes after lumbar discectomy for sciatica: the effects of fragment type and anular competence. J Bone Joint Surg Am. januar 2003;85(1):102–8.
42. Gupta A, Upadhyaya S, Yeung CM, Ostergaard PJ, Fogel HA, Cha T, mfl. Does Size Matter? An Analysis of the Effect of Lumbar Disc Herniation Size on the Success of Nonoperative Treatment. Glob Spine J. 1. oktober 2020;10(7):881–7.
43. Lønne G, Solberg TK, Sjaavik K, Nygaard ØP. Recovery of muscle strength after microdiscectomy for lumbar disc herniation: a prospective cohort study with 1-year follow-up. Eur Spine J. april 2012;21(4):655–9.
44. Jesson T. Sciatica – The clinician’s guide. Book 1: What is it? 2021.
45. Brock M, Patt S, Mayer HM. The form and structure of the extruded disc. Spine. desember 1992;17(12):1457–61.
46. Bouma GJ, Barth M, Ledic D, Vilendecic M. The high-risk discectomy patient: prevention of reherniation in patients with large anular defects using an anular closure device. Eur Spine J. mai 2013;22(5):1030–6.
47. Carragee EJ, Spinnickie AO, Alamin TF, Paragioudakis S. A prospective controlled study of limited versus subtotal posterior discectomy: short-term outcomes in patients with herniated lumbar intervertebral discs and large posterior anular defect. Spine. 15. mars 2006;31(6):653–7.
48. Parker SL, Mendenhall SK, Godil SS, Sivasubramanian P, Cahill K, Ziewacz J, mfl. Incidence of Low Back Pain After Lumbar Discectomy for Herniated Disc and Its Effect on Patient-reported Outcomes. Clin Orthop Relat Res. juni 2015;473(6):1988–99.
49. As R, S K, Tk S, I A, Ji B, Fc D, mfl. Impact of the number of previous lumbar operations on patient-reported outcomes after surgery for lumbar spinal stenosis or lumbar disc herniation. Bone Jt J [Internett]. 15. mars 2023 [sitert 12. februar 2025];105-B(4). Tilgjengelig på: https://pubmed.ncbi.nlm.nih.gov/36924173/
50. Lebow RL, Adogwa O, Parker SL, Sharma A, Cheng J, McGirt MJ. Asymptomatic same-site recurrent disc herniation after lumbar discectomy: results of a prospective longitudinal study with 2-year serial imaging. Spine. 1. desember 2011;36(25):2147–51.
51. Helseth Ø, Lied B, Halvorsen CM, Ekseth K, Helseth E. Outpatient Cervical and Lumbar Spine Surgery is Feasible and Safe: A Consecutive Single Center Series of 1449 Patients. Neurosurgery. juni 2015;76(6):728–37; discussion 737-738.
52. Park C, Garcia AN, Cook C, Gottfried ON. Effect of change in preoperative depression/anxiety on patient outcomes following lumbar spine surgery. Clin Neurol Neurosurg. 1. desember 2020;199:106312.
53. Jackson KL, Rumley J, Griffith M, Agochukwu U, DeVine J. Correlating Psychological Comorbidities and Outcomes After Spine Surgery. Glob Spine J. oktober 2020;10(7):929–39.
54. Currie SR, Wang J. More data on major depression as an antecedent risk factor for first onset of chronic back pain. Psychol Med. september 2005;35(9):1275–82.
55. Carreon LY, Jespersen AB, Støttrup CC, Hansen KH, Andersen MO. Is the Hospital Anxiety and Depression Scale Associated With Outcomes After Lumbar Spine Surgery? Glob Spine J. mai 2020;10(3):266–71.
56. Sullivan MJL, Tripp DA. Pain Catastrophizing: Controversies, Misconceptions and Future Directions. J Pain. 1. mars 2024;25(3):575–87.
57. Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing: a critical review. Expert Rev Neurother. mai 2009;9(5):745–58.
58. Martinez-Calderon J, Jensen MP, Morales-Asencio JM, Luque-Suarez A. Pain Catastrophizing and Function In Individuals With Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Clin J Pain. mars 2019;35(3):279–93.
59. Sullivan MJL, Bishop SR, Pivik J. The Pain Catastrophizing Scale: Development and validation. Psychol Assess. 1995;7(4):524–32.
60. Kim HJ, Park JW, Chang BS, Lee CK, Yeom JS. The influence of catastrophising on treatment outcomes after surgery for lumbar spinal stenosis. Bone Jt J. november 2015;97-B(11):1546–54.
61. Tuna T, Boz S, Van Obbergh L, Lubansu A, Engelman E. Comparison of the Pain Sensitivity Questionnaire and the Pain Catastrophizing Scale in Predicting Postoperative Pain and Pain Chronicization After Spine Surgery. Clin Spine Surg. november 2018;31(9):E432–40.
62. Fernandes L, Storheim K, Lochting I, Grotle M. Cross-cultural adaptation and validation of the Norwegian pain catastrophizing scale in patients with low back pain. BMC Musculoskelet Disord. 22. juni 2012;13:111.
63. Petrini L, Arendt-Nielsen L. Understanding Pain Catastrophizing: Putting Pieces Together. Front Psychol. 2020;11:603420.
