A few years ago, as a novice clinician, I believed that physiotherapy could fix everything and that no one really needed surgery. Disc herniations didn’t cause any trouble, just look at how many asymptomatic individuals have them. Why even consider surgery at all? I hesitated to use the term “herniation” because I’d heard that it could instill more fear and pain in the patient. I’ve grown a few years older and now I’m not afraid to tell someone that they likely have a disc herniation with radicular pain, and I’ve come to understand that a few people actually require surgery.
Why know something about this?
We know of course that disc changes are a normal part of aging, just like wrinkles, but sometimes particular changes can cause some trouble. When the patient comes see you with the MRI results in his hand it is important to know the terminology, so that you can actually know if the subjective and objective matches up with the MRI results, and then use this to give the patient an up-to-date explanation. Probably nine out of ten times it will mean cognitive reassurance (they should maybe not have had the MRI in the first place?), but a few times the changes, f.ex. a disc extrusion in a posterolateral localisation can cause radicular pain and radiculopathy. Knowing about this makes it easier for your clinical reasoning.
What’s the definition?
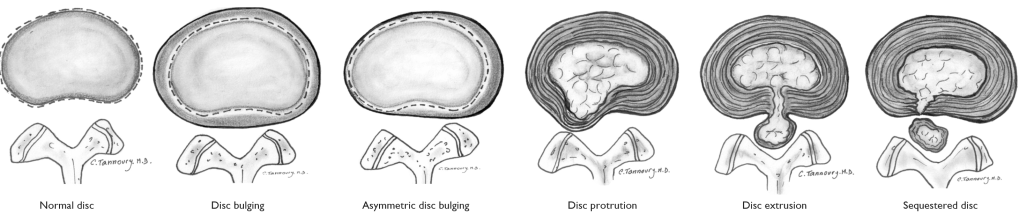
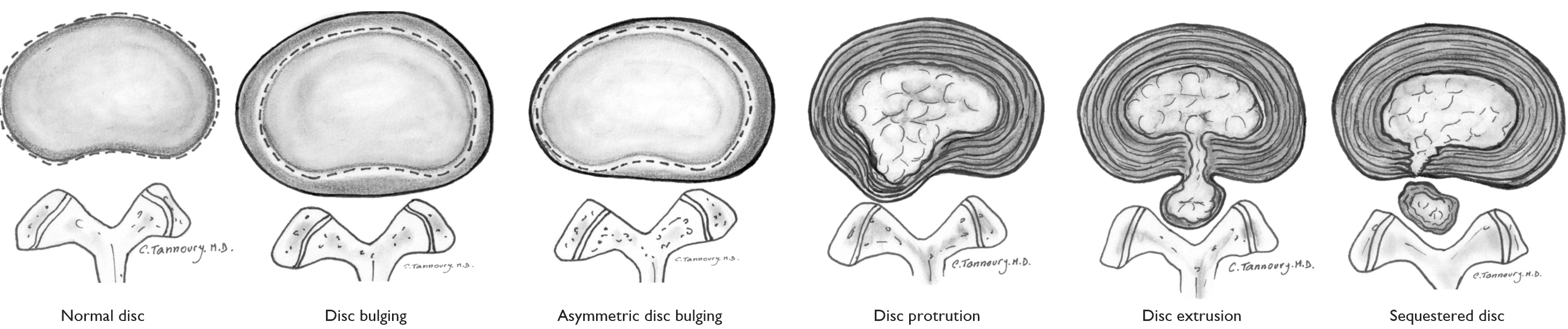
Is disc protrusion the same as disc herniation? What about disc bulge? Extrusion? Sequestration? Fortunately, there are those who have taken on the task of clearing this up. The article “Lumbar Disc Nomenclature: Version 2.0” defines what constitutes a normal disc, disc bulging, disc protrusion, disc extrusion and sequestered disc as seen on MRI (1).
Note: Remember I am mostly talking about definitions and terminology in this article, not too much about pain. Disc changes are of course normal, they’re just like wrinkles on the inside, but some changes can also increase the chance of getting pain, like f.ex. a disc extrusion. Therefore it is important to know the terminology, so to better understand what’s going on.
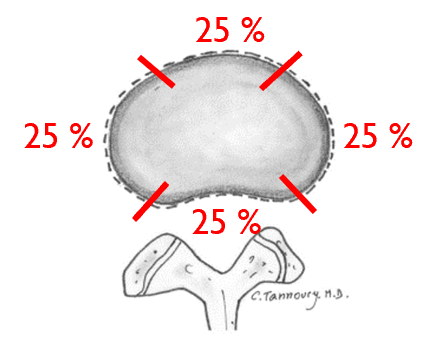
The actual definition of a disc herniation is as follows (1):
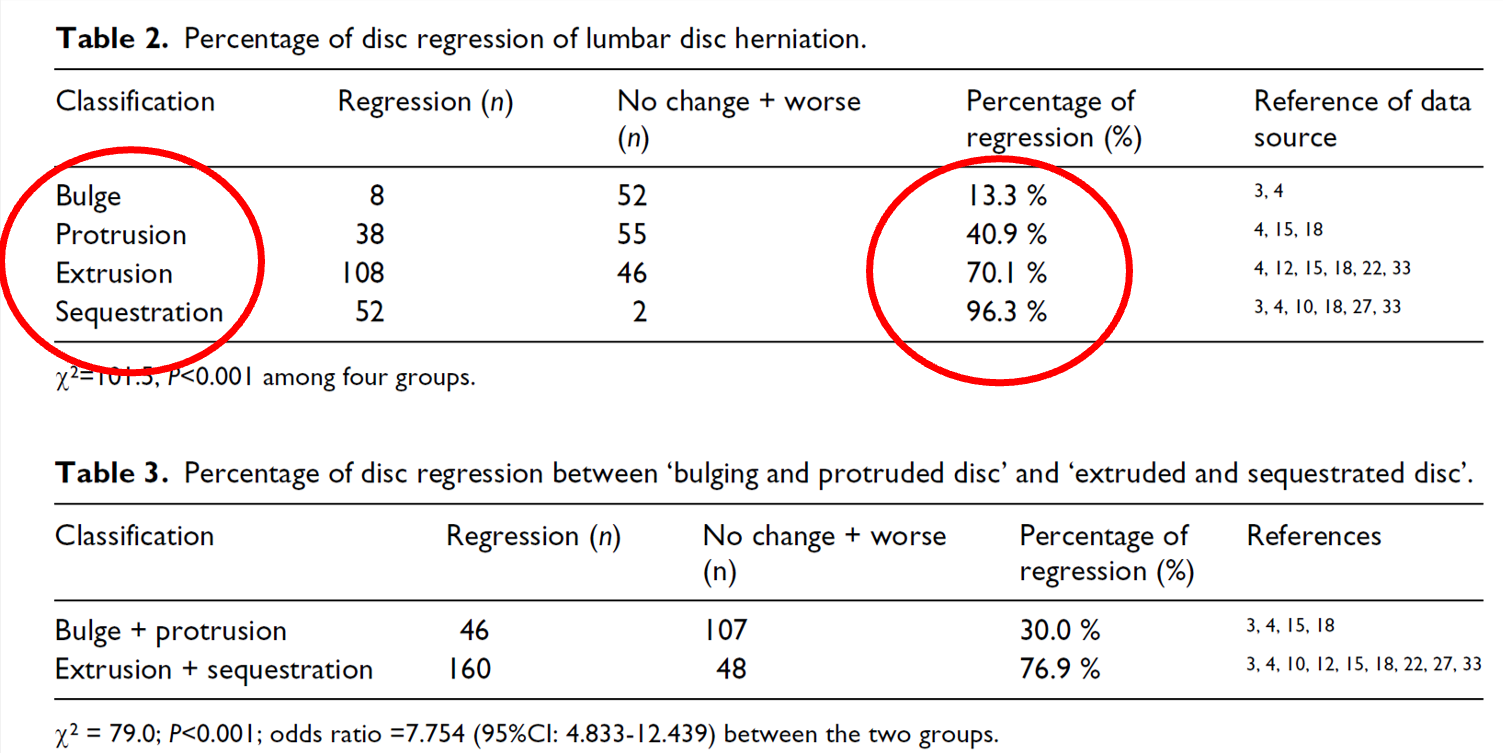
A disc herniation is a localized displacement of material. “Less than 25% of the circumference” means that it “sticks out” in a maximum of one-quarter of the edge (see the image below for clarification). A disc bulge will “protrude” more than 25%, hence it is not a herniation. A disc herniation can be both a protrusion (the herniation base is thicker/wider than the herniation head) and an extrusion (the herniation head is thicker/wider than the herniation base) (1). Whether it is called an extrusion or a protrusion does not indicate whether it has breached the wall or not, but an extrusion has more often breached the wall than a protrusion. A sequestered herniation refers to disc material that has become detached from the disc. This means that protrusion, extrusion, and sequestered disc are all herniations, while disc bulge is not.
One can also use the terms “contained” and “uncontained.” A disc herniation is contained if it is located within the annulus or posterior longitudinal ligament, meaning it has not breached the wall. If it has breached the wall, then it is uncontained. A disc herniation is not necessarily just a displacement of nucleus pulposus material; it can also involve cartilage and other fragmented tissue (1). Therefore, it is incorrect to label it as herniation of the nucleus pulposus.
Why is it important to know, you say? Because the body’s defense system is more activated and wants to fix stuff if it notices something that is not supposed to be there, f.ex. disc material in the spinal canal.
Location and size
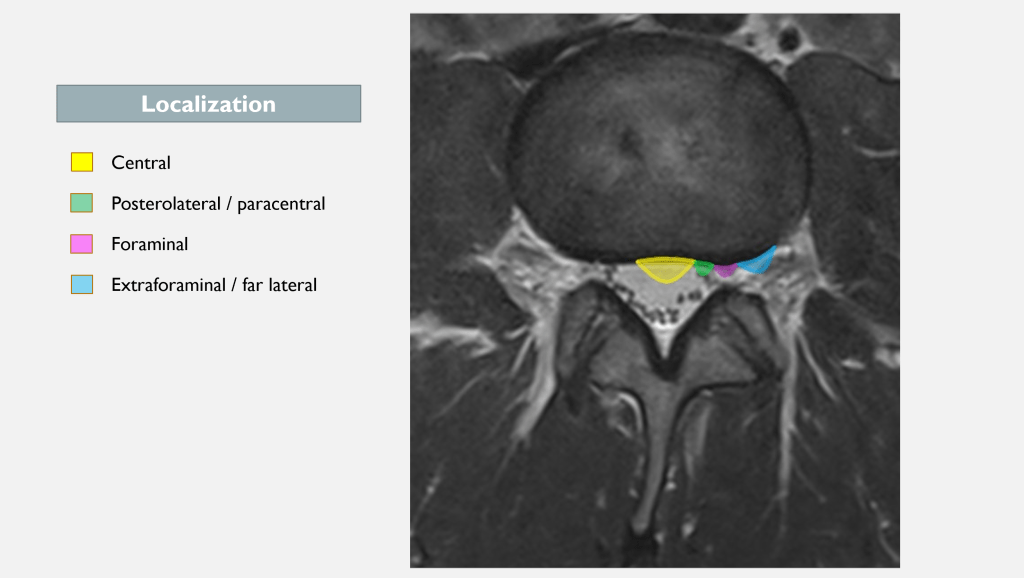
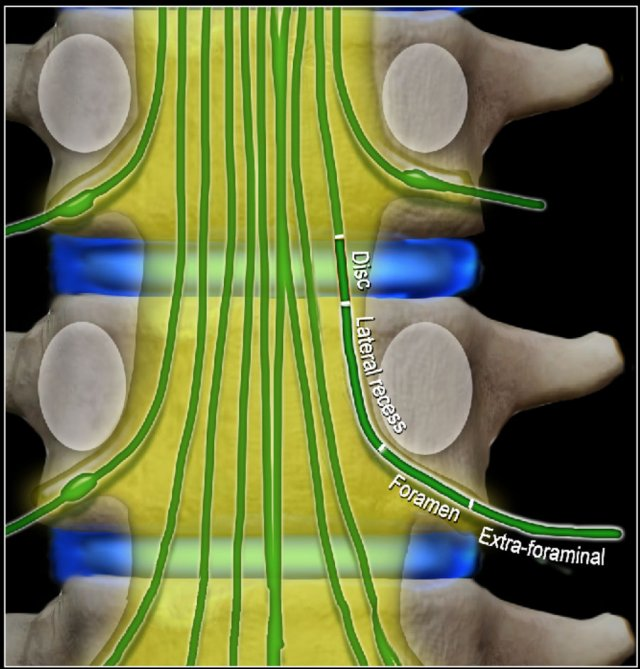
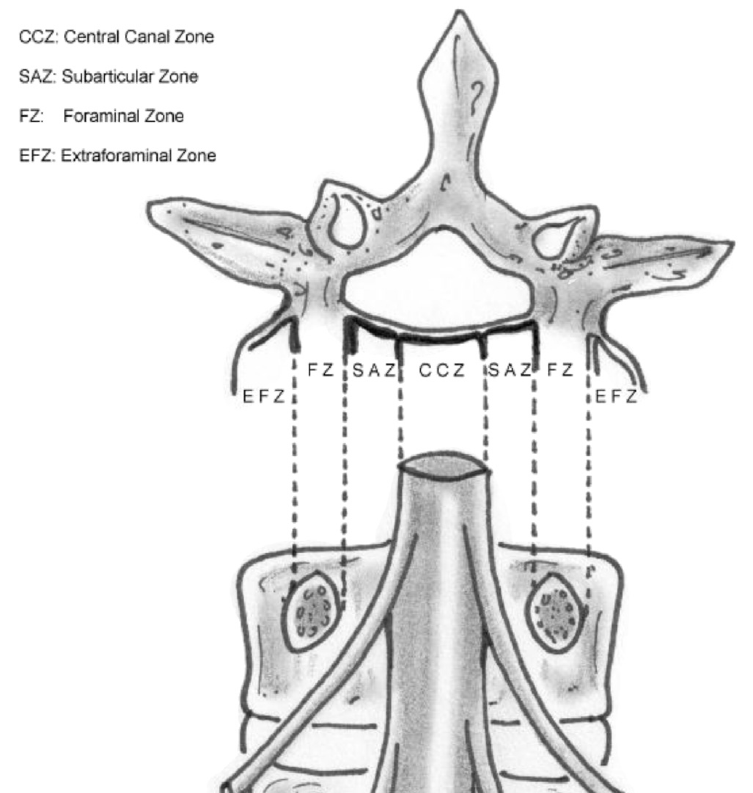
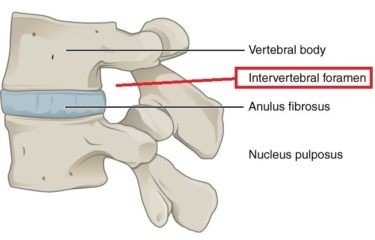
An easy way to classify disc herniations is: Central (medial), paracentral (posterolateral), and foraminal or extraforaminal (far lateral) (3).
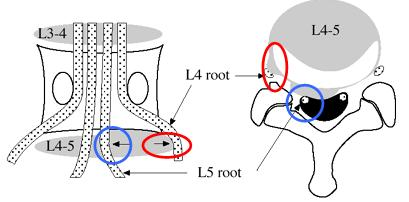
Where the herniation is located is crucial for determining which structures it could potentially affect. For instance, a paracentral L4-5 disc herniation could impact the L5 nerve root, but if it’s positioned slightly more laterally, in the intervertebral foramen, it could affect the L4 nerve root (see image below).
Note: The nerve root is also referred to as the spinal nerve. It becomes a nerve root/spinal nerve only when it exits the central nervous system, i.e., the spinal cord.
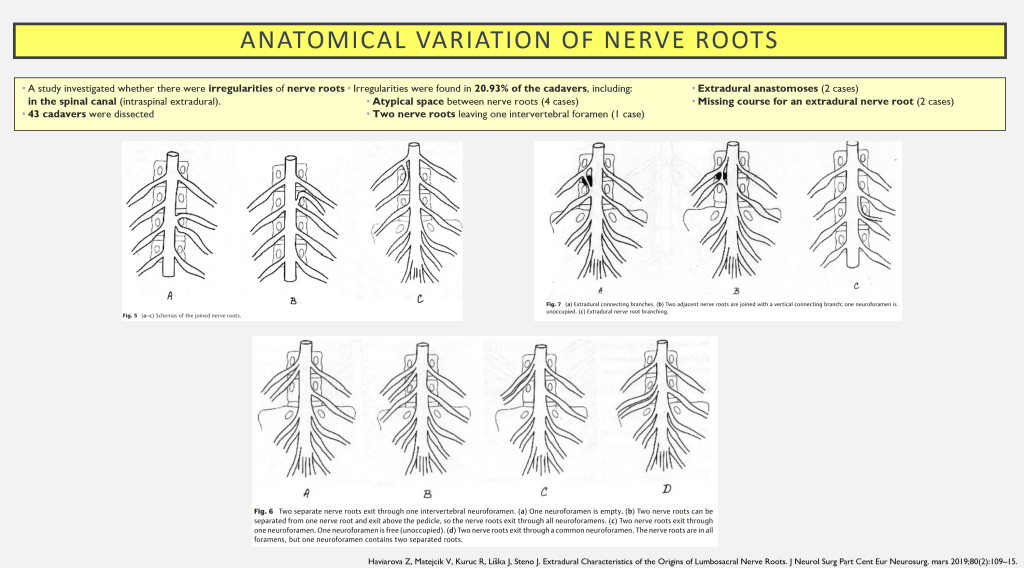
An important point here is the normal variation in the pathways of nerve roots. A study found irregularities in 1/5 of the nerve roots in dissected cadavers (17).
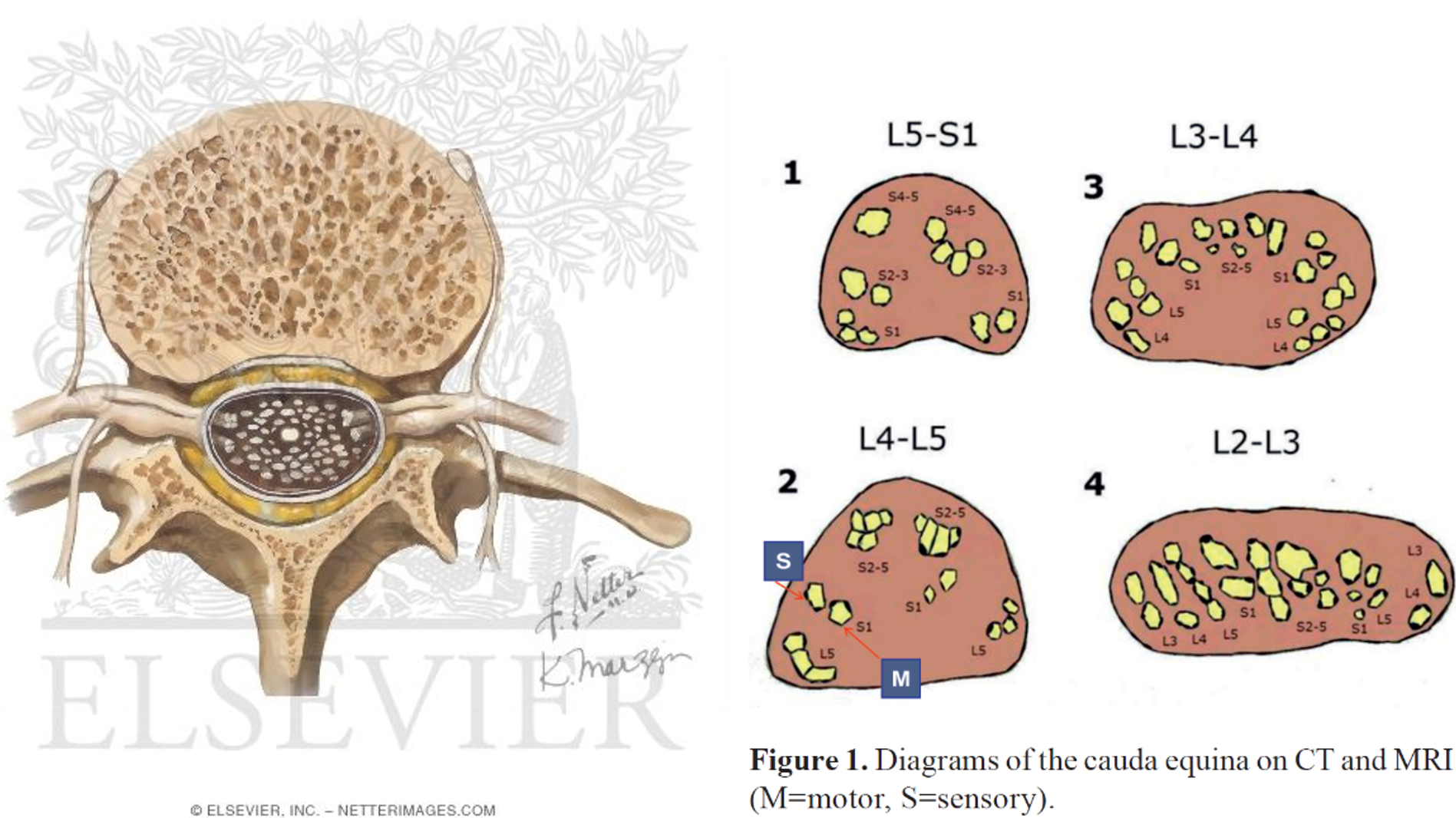
The nerve roots in the lower back must cover a longer distance, like a horse’s tail, before they exit through the intervertebral foramen and the foramina sacralia anteriora, because the spinal cord ends at approximately L2 (4). One might think that a herniation at L4/L5 would compress the spinal cord, but no, it compresses the cauda equina – the horse’s tail. The cauda equina/nerve roots also don’t resemble the anatomical models (18). This can contribute to confusion when assuming that a disc herniation in a certain location would press on a specific nerve.
Multiple nerve roots can be affected by a large disc herniation in the lower back, especially a significant central herniation that could lead to cauda equina syndrome (CES), though only two percent (?) of disc herniations progress to become CES (5).
Note: It is recommended saying the “subarticular recess/zone” instead of the “lateral recess”. But people will probably still use “the lateral recess”, because it is a more well known term
For an even more detailed description of localization, one can again refer to the “golden standard” (1), although this has also been debated (6).
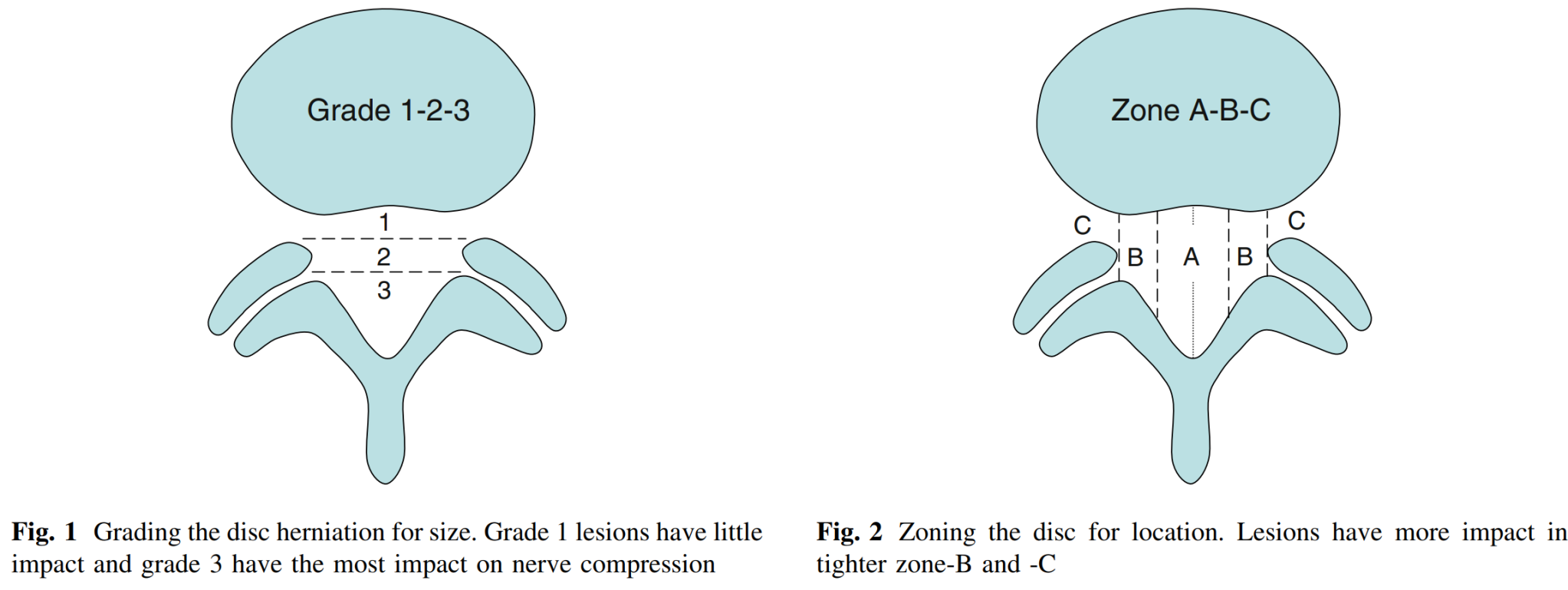
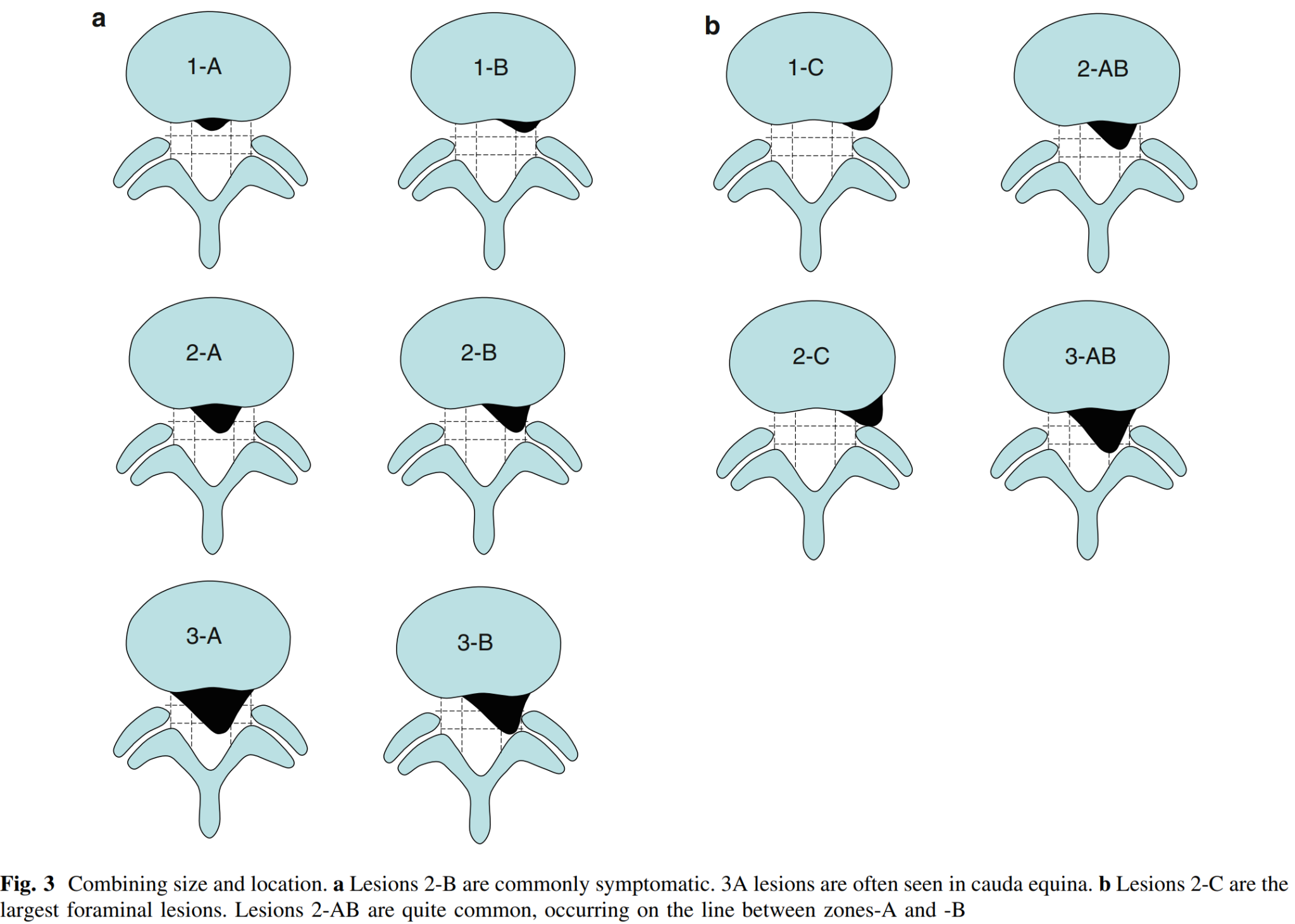
A framework that combines both localization and size has also been proposed, known as the MSU Classification for herniated lumbar discs on MRI. Size is categorized as grade 1, 2, or 3, and localization as zone A, B, or C, and these can also be combined (7).
In this study of 181 patients who underwent surgery for disc herniation, they found that the majority were of type 2-B and 2-AB (8). This aligns with other research indicating that over three-quarters of disc herniations occur paracentrally (posterolaterally) (8). In this region, the annulus fibrosus is thinner and lacks support from the posterior longitudinal ligament. The distance to the nerve root is short (9). Many type 2-A disc herniations that extend directly into the spinal canal can be less symptomatic and more suitable for conservative treatment. Localization and size are significant factors (7).
Foraminal and extraforaminal disc herniations, in zone C, are rarer (7-12% / 21%) compared to central and paracentral herniations (10). As mentioned, these herniations can affect the nerve root at the same level where it exits through the intervertebral foramen. Patients with these herniations might experience more pronounced symptoms, as disc material can protrude into a narrower canal with limited space for nerve displacement. The dorsal root ganglion is also located in this area, which is a potentially pain-sensitive structure (11,12).
A study confirms this, as patients with foraminal and extraforaminal herniations had more radiating leg pain compared to those with central and paracentral herniations (10). One would also expect these patients to experience more frequent or severe muscle weakness. However, two studies on this topic provide conflicting answers (10,13). Patients with foraminal and extraforaminal herniations are on average older (with age differences of 8.6, 8.2, and 1.87 years in three studies) (10,13,14). These herniations can be somewhat more challenging to diagnose, as the positive Lasègue test is less common. It appears that these patients have somewhat poorer outcomes from both surgery and conservative treatment (10,14).
Where do disc herniations most commonly occur?
Nearly all (95%) of disc herniations occur in the two lower discs of the lumbar spine, L4/L5 and L5/S1. Patients are typically between 30-50 years old, and the male-to-female ratio is 2:1. Herniations above the two lower discs are more common in individuals over 55 years old (15). In observational studies, there is no significant relationship between the level of disc herniation and prognosis after 8 years (16).
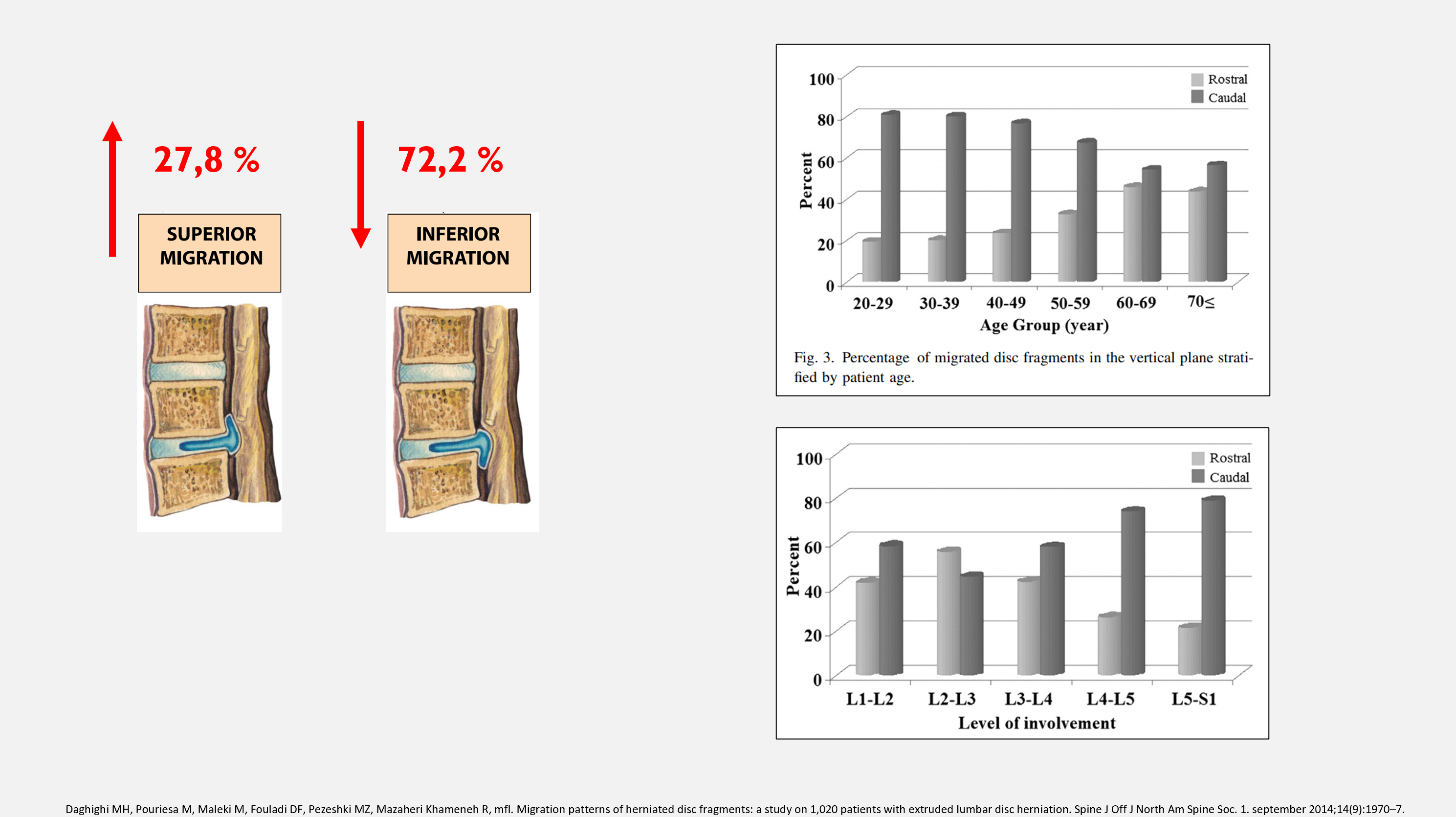
Most disc herinations migrates inferiorly
Summary
A herniation is a localized displacement of material, which can include protrusion, extrusion, and sequestration. A disc herniation has the potential to affect multiple nerve roots depending on its location. In 3/4 of cases, herniations occur paracentrally/posterolaterally, and 95% of lumbar disc herniations occur in the two lower discs.
References
1. Fardon DF, Williams AL, Dohring EJ, Murtagh FR, Gabriel Rothman SL, Sze GK. Lumbar disc nomenclature: version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Spine J Off J North Am Spine Soc. 1. november 2014;14(11):2525–45.
2. Adams MA, editor. The biomechanics of back pain. 3rd ed. Edinburgh ; New York: Churchill Livingstone/Elsevier; 2013. 335 s.
3. Eck JC, Vaccaro AR, Jaypee Brothers Medical Publishers. Surgical atlas of spinal operations. New Delhi [etc.: Jaypee Brothers Medical Publ.; 2013.
4. Jansen J, Dietrichs E, Holck P. cauda equina. I: Store medisinske leksikon [Internett]. 2019 [sitert 23. mars 2020]. Tilgjengelig på: http://sml.snl.no/cauda_equina
5. Greenhalgh S, Truman C, Webster V, Selfe J. An Investigation into the Patient Experience of Cauda Equina Syndrome (CES). Physiother Pract Res. 1. januar 2015;36:23–31.
6. Li Y, Fredrickson V, Resnick DK. How should we grade lumbar disc herniation and nerve root compression? A systematic review. Clin Orthop. juni 2015;473(6):1896–902.
7. Mysliwiec LW, Cholewicki J, Winkelpleck MD, Eis GP. MSU Classification for herniated lumbar discs on MRI: toward developing objective criteria for surgical selection. Eur Spine J. juli 2010;19(7):1087–93.
8. Lurie JD, Tosteson TD, Tosteson ANA, Zhao W, Morgan TS, Abdu WA, mfl. Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial. Spine. 1. januar 2014;39(1):3–16.
9. Dulebohn SC, Ngnitewe Massa R, Mesfin FB. Disc Herniation. I: StatPearls [Internett]. Treasure Island (FL): StatPearls Publishing; 2020 [sitert 23. mars 2020]. Tilgjengelig på: http://www.ncbi.nlm.nih.gov/books/NBK441822/
10. Lee JH, Lee S-H. Clinical and Radiological Characteristics of Lumbosacral Lateral Disc Herniation in Comparison With Those of Medial Disc Herniation. Medicine (Baltimore) [Internett]. 18. februar 2016 [sitert 23. mars 2020];95(7). Tilgjengelig på: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4998615/
11. Epstein NE. Foraminal and far lateral lumbar disc herniations: surgical alternatives and outcome measures. Spinal Cord. oktober 2002;40(10):491–500.
12. Park HW, Park KS, Park MS, Kim SM, Chung SY, Lee DS. The Comparisons of Surgical Outcomes and Clinical Characteristics between the Far Lateral Lumbar Disc Herniations and the Paramedian Lumbar Disc Herniations. Korean J Spine. september 2013;10(3):155–9.
13. Mérot OA, Maugars YM, Berthelot J-MM. Similar outcome despite slight clinical differences between lumbar radiculopathy induced by lateral versus medial disc herniations in patients without previous foraminal stenosis: a prospective cohort study with 1-year follow-up. Spine J Off J North Am Spine Soc. 1. august 2014;14(8):1526–31.
14. Khan JM, McKinney D, Basques BA, Louie PK, Carroll D, Paul J, mfl. Clinical Presentation and Outcomes of Patients With a Lumbar Far Lateral Herniated Nucleus Pulposus as Compared to Those With a Central or Paracentral Herniation. Glob Spine J. august 2019;9(5):480–6.
15. Jordan J, Konstantinou K, O’Dowd J. Herniated lumbar disc. BMJ Clin Evid. 26. mars 2009;2009.
16. Kerr D, Zhao W, Lurie JD. What Are Long-term Predictors of Outcomes for Lumbar Disc Herniation? A Randomized and Observational Study. Clin Orthop. juni 2015;473(6):1920–30.
17. Haviarova Z, Matejcik V, Kuruc R, Líška J, Steno J. Extradural Characteristics of the Origins of Lumbosacral Nerve Roots. J Neurol Surg Part Cent Eur Neurosurg. mars 2019;80(2):109–15.
18. Kapetanakis S, Chaniotakis C, Kazakos C, Papathanasiou JV. Cauda Equina Syndrome Due to Lumbar Disc Herniation: a Review of Literature. Folia Med (Plovdiv). 20. desember 2017;59(4):377–86.